20 years ago today (I started writing this on May 27th), I stopped taking health for granted. It would be another decade before life as I knew it abruptly disappeared with the collapse of my immune system and the descent into severe ME/CFS, but this day in 2001 was the beginning of the end of health ignorance and body confidence.
My husband and I were at my friend’s birthday party, sitting at an outdoor table in the dark, chatting, drinking beers, smoking cigarettes. My breathing started bothering me to the point that I mentioned it to my boyfriend (at the time). He put his ear on my chest and said he didn’t hear anything abnormal. But that’s why it got my attention — I’d had many, many chest infections and asthma issues in my life, but this was different, this was like a vice around my lungs. I was smoking, though, so it was easy to explain away. And I was drinking, so I didn’t want the party to stop.
A while later, I went to the bathroom and, when I looked in the mirror, I saw a huge defined rash on the bottom of my face, down my neck and onto my chest. It looked like I’d drawn a distinct outline and colored it in with a bright red marker. I’d never, ever dealt with hives or rashes and I always thought they were blotchy and maybe raised, maybe itchy. This was nothing like that; this looked like a slab of raw steak.
We decided to go home and, on the way, I called the consulting nurse service at my doctor’s clinic. The nurse asked me if my tongue was swollen and I replied: “Yeah, actually, it’s so big, I’m chewing on it. “ She very calmly said: “Hang up the phone and call an ambulance.” When my boyfriend heard this, he turned around and drove through every red light to get to the emergency room. It was such a weird experience — the triage nurse took one look at me and brought me straight back to get hooked up to an IV. I was drunk, totally oblivious to the seriousness of the situation and then quickly doped up on diphenhydramine and mellow. Before we went home, the nurse said it was the worst case of anaphylaxis she’d ever seen.
But when you’re young and healthy, it’s easy to ignore these things. It happened twice more before I went to see a specialist and all the RAST and typical allergy blood tests came back negative. I told the doctor that every time it happened, I was at an event or party (after the first birthday party, it happened at another birthday party, an Oktoberfest gathering and an Easter celebration), I had been drinking alcohol and it was the start of my period. Those were the common denominators. I was dismissed by the allergist at the University of Washington Medical Center — he actually threw the Pub Med articles that I had printed out at the library into the trash can in front of me with a flourish — and so I dismissed it, too. They know best, right?
The last time I went into full-blown, classic-presenting anaphylaxis, I almost died. I was a rag doll, carried down the stairs on a stretcher by the paramedics. They kept asking what drugs I had taken, not believing that this was an “anaphylactic reaction to alcohol.” It traumatised my boyfriend and mother. It was the last time I had a drop of booze.
My body, my health, and our lives have never been the same. 20 years of collapses and tests, specialists, diagnoses, treatments and medications, pain, reactions, research, fear, loss of career, social life and hopes for the future.
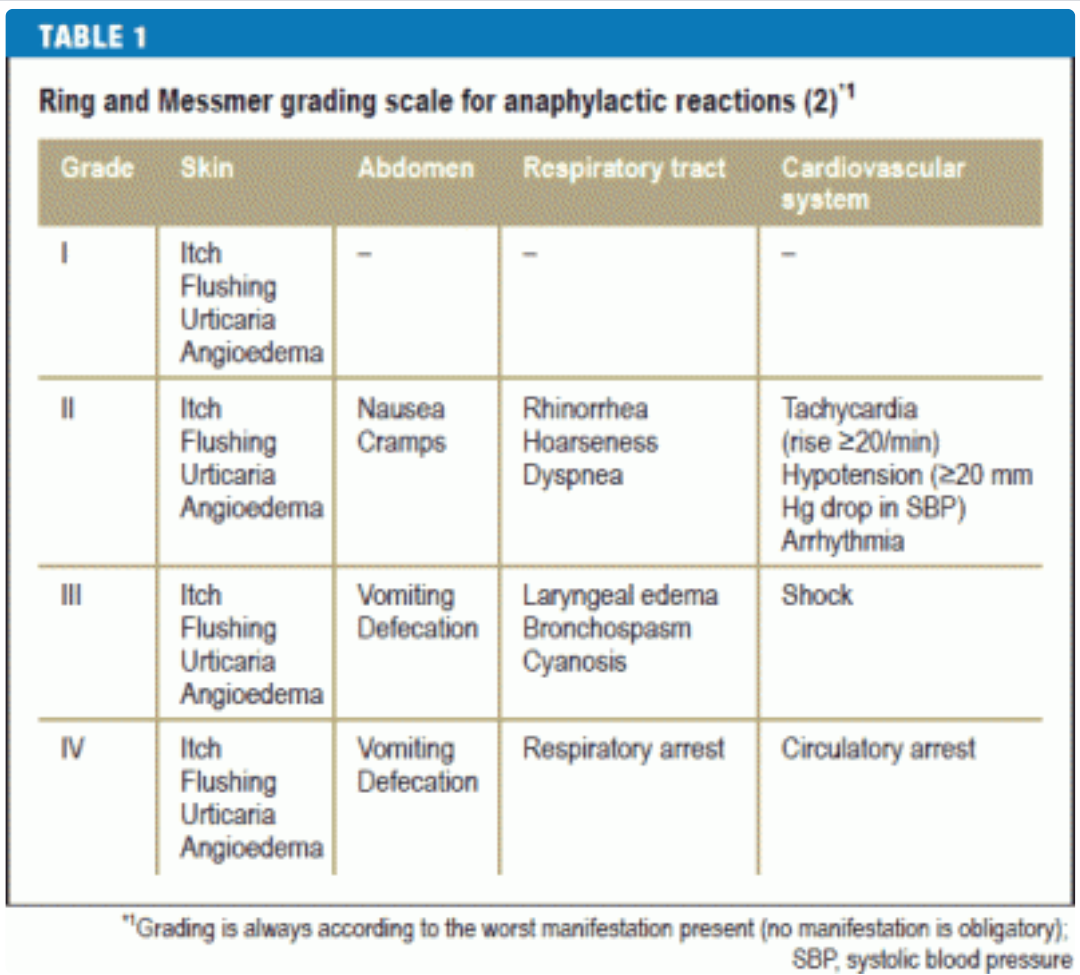
I haven’t gone into grade III anaphylaxis (bordering on grade IV that last time) since 2002, but the spectre is always there. Hypotension, heart arrhythmias, angioedema — they’re barely managed and always providing a low-level thrum of unease in my days. I could escalate at any time if you’re not hypervigilant, they say. But I’m not very careful and I like to test the boundaries. I found over the years that the negative effects from hypervigilance just slightly outweigh the fear that is borne of risk-taking, especially when each time I throw caution to the wind and come out unscathed, I gain a little bit of confidence and hope that I’m safe now and it won’t happen again.
I don’t do parties, though, and I try to keep menstruation at bay with prescription hormones. And I’ll never have another drink as long as I live, even if I woke up healthy tomorrow. My mast cells will continue to find new and creative ways to wreak havoc on my body without my help.