A decade since my body and health were not on my mind.
A decade since my last cold, flu or bronchitis.
A decade since my last vaccination.
A decade since I enjoyed Halloween, my favourite holiday.
A decade since I was in a lake or ocean.
A decade since I was on a train.
A decade since I stood up at a concert.
A decade since I didn’t wear a mask on a plane.
A decade since I went to a wedding.
A decade since I went to a barbecue.
A decade since seeing so many friends.
A decade since I married my longtime boyfriend because “I feel like something is going to happen to me and I want you to be able to legally speak for me, if I can’t speak for myself.”
A decade since I was in Ireland, in my childhood home, walking the streets of my heart.
I thought about this anniversary so many times in the past. For a long time, I thought there was no way it would come–I couldn’t possibly stay sick this long. Every other illness had a beginning and an end, so, surely, one day my body would recover and this spectre would leave, it was just taking a little longer than the usual virus.
Once I realised it was lifelong, I thought the 10-year mark would be a momentous and heavy occasion. It turns out, it’s not. 2 years seemed much harder to accept. Back when isolation was still harrowing and loneliness still suffocated. You get used to both. It helps if you can develop a deep disdain for humans, so you can trick yourself into believing you’re not missing out on anything. And the 5-year mark was hard. I’d felt small, but miraculous changes from IVIG and then had an epic autumn backslide that year. The dowsing of that little flame of hope was devastating and it was inconceivable that I would be physically or mentally resilient enough to continue the maybe-I’m-getting-better!-Oh-no-what-fresh-hell-is-this? cycle for years to come.
But, then, suddenly, 10 years have passed. I could almost believe the rest of the world is trapped in amber, frozen in time, awaiting my return. As soon as I kick this thing, I’ll drive back down to the office–each street scene melting and returning into motion as my car passes by–and get back to work. Thanks for waiting, guys.
INFECTIONS
What’s far more unbelievable to me is that I haven’t had a muggle illness in a decade. [Please don’t let this jinx me.] No head cold, no flu, no stomach bug, no chest/ear/sinus/bladder/any-other-part-of-the-body infection. The more time that went by, the more ominous was the thought of contracting an acute virus. For years, I had relentless flu-y symptoms–headaches, sore throats, muscle pain, weakness, chills (and still do, sporadically)–and I have many high out-of-range infection titers*, so the thought of another malady compounding the daily slog was harrowing.
*HHV6 IgG; HSV IgM; EBV IgG; M Pneumoniae IgG; S. Cerevisiae IgG; Varicella IgG and IgM; Coxsackie A7, A9, A16, A24, B1, B2, B5 and B6; Anti Streptolysin O Titer, and Candida IgM and IgA. Yes, really.
Three years into my illness, Dr. Chia told us unequivocally that a run-of-the-mill cold could make me permanently worse, so we have always taken great precautions to avoid exposure, which have only intensified during this pandemic. I honestly wonder if I’ll ever be indoors and maskless with anyone besides my husband again. Even worse, will my husband ever be indoors and maskless with anyone besides me? It’s one thing to choose this life for myself–I’ve made peace with only having remote communication with friends and family; I have a partner and a dog to keep me sane–but my healthy husband’s life has shriveled to keep me safe and the guilt from that is indescribable. I imagine if he weren’t yoked to someone at such risk for serious complications from viruses, he might be out gallivanting and socialising, as well he should be.
VACCINES
One of the first doctors I saw after falling ill said, “You are very sick. We don’t know what’s wrong with you, but you should never get another vaccination as long as you live.” I was confused because, until that moment, I hadn’t linked whatever this sickness was to the flu shot I’d gotten a week before Halloween. I was also confused because, in my healthy ignorance, I thought vaccines only bolstered your immune system. I really didn’t understand, in certain unique circumstances, that they could break it. I used to get every immunization available in an effort to protect myself.
Before I traveled to Central America, I was vaccinated for polio, live typhoid, hepatitis A and B, tetanus, diphtheria and gammastan–all on the same day. In the years after, I got the live varicella vaccine, the 3-shot hepatitis B series, measles, mumps, and rubella and, of course, the flu shot every year, along with a pandemic flu vaccine (H1N1) when they were offered. I didn’t get majorly sick while traveling, I didn’t get chicken pox when I tended to my horrifically poxy husband and I never got the flu despite working very long hours in restaurants, among infectious people (note to the public: restaurant staff work when they’re sick; you have to be on death’s door to ask someone to cover a shift), so I guess the vaccines helped… until they harmed.
COVID
There’s such polarization these days when it comes to covid vaccines. There’s a lot of hatred directed at those who are trying to protect themselves and others by getting vaccinated and wearing masks and there is an equal amount of contempt directed at anti-vaxers. I have yet to see a single news story talk about those of us who want to get vaccinated, but cannot. Or those of us who have to make the agonizing decision to live a life of extreme isolation or risk very serious repercussions from a vaccine–any vaccine. I wish individuals would always take the collective into consideration and try to protect those that are vulnerable, but that’s not human nature, unfortunately. People will refuse vaccinations or not wear masks or not get tested because they don’t want to quarantine. And, all the while, those of us with weakened, damaged or overactive immune systems–be it from chemo or old age or autoimmunity or ME/cfs or steroids or stress or another condition–will have to choose seclusion over risk.
Against one of my doctor’s advice, I will be getting the first covid vaccine next month–but I’m getting a pediatric dose. We will see how I do and then I’ll get a second dose and test antibodies. They will be keeping me for observation in the clinic for an hour because of my history of anaphylaxis, but that’s not what I’m worried about.
I’m worried about being bedbound again. I’m worried about volunteering for an injection that could further damage my autonomic nervous system and intensify dysautonomia and hyperadrenergic symptoms. I’m worried about triggering more vasovagal collapses or making myself more hemodynamically unstable. I’m worried about a cytokine storm and/or a mast cell meltdown that creates a permanent worsening of reactivity when I’m already so limited in medication options and trying so hard to keep on weight. I’m worried about a blood clot causing sudden death because IVIG, oral hormones and inactivity already put me in a high-risk category. I’m worried about losing the limited amount of independence and mobility I have now (but it’s enough for a happy life) and becoming too weak to even wash my hair again. I’m worried about being that burden to my husband again, especially now that it takes so much work to make my GI tract function–it would be a monstrous task for him to take on. Mostly, I’m worried about once again losing the small joys, like taking Penny on our scooter walks, being able to talk on the phone for hours and laughing. I spent years without those gifts and I’m not sure I can claw my way back over another decade.
It feels good to write out those fears. There are very few people with whom I can have these discussions because not many healthy friends understand the risks involved when dealing with such complex conditions. Everyone in my family has had at least 2 covid vaccinations with no side effects, but, in my support groups, it’s a different story. Even there, though, I am careful–I want everyone to get vaccinated, if they can safely, and I never want to dissuade others by voicing my concerns. And doctors aren’t much help because the vast majority take the practical stance that, statistically, the chances of negative repercussions are low and that the risks outweigh the benefits. That’s absolutely true for the typical bell curve of the typical population. Not true for me.
Let’s just hope it’s all smooth sailing. I’d like the next decade to be different.
Update: My doctor pretty much talked me out of getting the C vaccine. I’m too high-risk for long-term reactions. I’m going to have to get surgery next year, so not being vaccinated in a hospital setting adds another layer of fear, but I won’t be stable enough for surgery if the vaccine caused damage. So I will be remaining in strict isolation and putting my life in other people’s hands.
20 years ago today (I started writing this on May 27th), I stopped taking health for granted. It would be another decade before life as I knew it abruptly disappeared with the collapse of my immune system and the descent into severe ME/CFS, but this day in 2001 was the beginning of the end of health ignorance and body confidence.
My husband and I were at my friend’s birthday party, sitting at an outdoor table in the dark, chatting, drinking beers, smoking cigarettes. My breathing started bothering me to the point that I mentioned it to my boyfriend (at the time). He put his ear on my chest and said he didn’t hear anything abnormal. But that’s why it got my attention — I’d had many, many chest infections and asthma issues in my life, but this was different, this was like a vice around my lungs. I was smoking, though, so it was easy to explain away. And I was drinking, so I didn’t want the party to stop.
A while later, I went to the bathroom and, when I looked in the mirror, I saw a huge defined rash on the bottom of my face, down my neck and onto my chest. It looked like I’d drawn a distinct outline and colored it in with a bright red marker. I’d never, ever dealt with hives or rashes and I always thought they were blotchy and maybe raised, maybe itchy. This was nothing like that; this looked like a slab of raw steak.
We decided to go home and, on the way, I called the consulting nurse service at my doctor’s clinic. The nurse asked me if my tongue was swollen and I replied: “Yeah, actually, it’s so big, I’m chewing on it. “ She very calmly said: “Hang up the phone and call an ambulance.” When my boyfriend heard this, he turned around and drove through every red light to get to the emergency room. It was such a weird experience — the triage nurse took one look at me and brought me straight back to get hooked up to an IV. I was drunk, totally oblivious to the seriousness of the situation and then quickly doped up on diphenhydramine and mellow. Before we went home, the nurse said it was the worst case of anaphylaxis she’d ever seen.
But when you’re young and healthy, it’s easy to ignore these things. It happened twice more before I went to see a specialist and all the RAST and typical allergy blood tests came back negative. I told the doctor that every time it happened, I was at an event or party (after the first birthday party, it happened at another birthday party, an Oktoberfest gathering and an Easter celebration), I had been drinking alcohol and it was the start of my period. Those were the common denominators. I was dismissed by the allergist at the University of Washington Medical Center — he actually threw the Pub Med articles that I had printed out at the library into the trash can in front of me with a flourish — and so I dismissed it, too. They know best, right?
The last time I went into full-blown, classic-presenting anaphylaxis, I almost died. I was a rag doll, carried down the stairs on a stretcher by the paramedics. They kept asking what drugs I had taken, not believing that this was an “anaphylactic reaction to alcohol.” It traumatised my boyfriend and mother. It was the last time I had a drop of booze.
My body, my health, and our lives have never been the same. 20 years of collapses and tests, specialists, diagnoses, treatments and medications, pain, reactions, research, fear, loss of career, social life and hopes for the future.
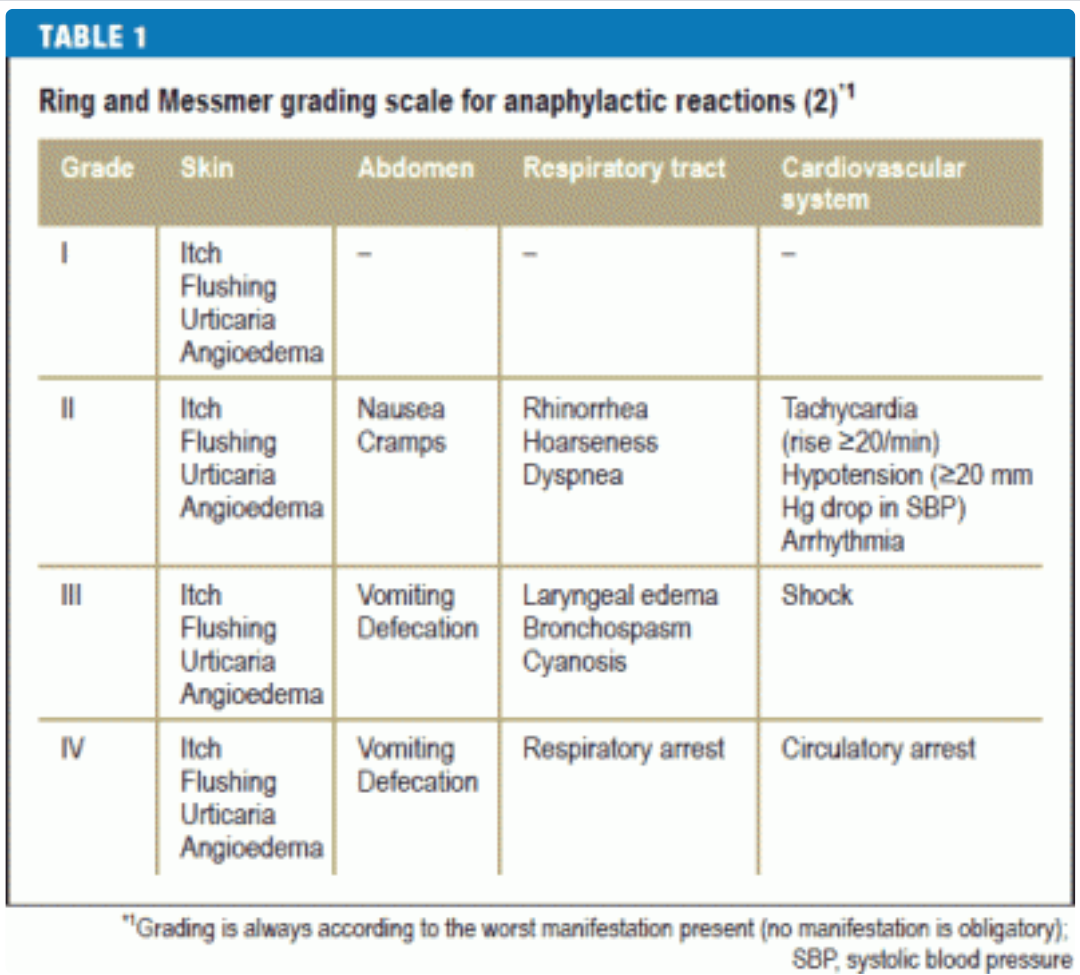
I haven’t gone into grade III anaphylaxis (bordering on grade IV that last time) since 2002, but the spectre is always there. Hypotension, heart arrhythmias, angioedema — they’re barely managed and always providing a low-level thrum of unease in my days. I could escalate at any time if you’re not hypervigilant, they say. But I’m not very careful and I like to test the boundaries. I found over the years that the negative effects from hypervigilance just slightly outweigh the fear that is borne of risk-taking, especially when each time I throw caution to the wind and come out unscathed, I gain a little bit of confidence and hope that I’m safe now and it won’t happen again.
I don’t do parties, though, and I try to keep menstruation at bay with prescription hormones. And I’ll never have another drink as long as I live, even if I woke up healthy tomorrow. My mast cells will continue to find new and creative ways to wreak havoc on my body without my help.
I want to talk about my success with IVIG (intravenous immune globulin) since this is something that I am frequently asked about by other patients. I’m in a very unusual situation where I administer my own IVIG and fluids through peripheral venous lines (not using a port or PICC) at home without a nurse. I feel extraordinarily fortunate to have been able to get this treatment at all, but it feels particularly fortifying during this pandemic. Not only because I am receiving a protective, difficult-to-access medication, but also because, when covid hit, I was in a position to continue treatment uninterrupted in my home without needing nursing visits that would increase my risk of exposure to the virus.
It’s also unusual that my IVIG is prescribed by a naturopath, rather than an MD (let alone an immunologist), and that I do infusions once a week rather than every 3 or 4 weeks, and that I was approved for a high ‘immunomodulatory’ dose without having one of the autoimmune diagnoses that is typically needed and without having to do a vaccine challenge. Also, I don’t have side effects from IVIG, which I find miraculous, but I think it is because of how careful (and controlling) I’ve been throughout the whole journey. I researched and advocated for myself at every turn — undoubtedly more than was really needed — but I have no regrets since it has been such a godsend and I’ve had no bad reactions.
The story starts when I went to see Dr. Chia in 2014 (almost 3 years after getting sick) and he ran a bunch of blood tests that no other doctor had bothered to explore up until that point, such as HHV6 and Coxsackie antibodies, T-cell counts, and total IgG with subclasses.
For anyone navigating the newly-sick morass, I want to point out that I had seen over 30 doctors in those first 3 years, trying desperately to find one big brain that might have some insight. Infectious disease, endocrinology, neurology, allergy, cardiology, rheumatology, sleep doctors, ENT, gastroenterology, functional medicine MDs — you are shunted from one specialty to another to another with no one willing to dig deeper. I am even including appointments with my OBGYN, ophthalmologist and acupuncturist in that count because I was chasing down every lead I could (maybe it’s all hormonal, maybe my eye pain will lead to a brain discovery, maybe ‘dark yin’ is my problem after all). The big issues were missed until I was able to see Dr. Chia and Dr. Kaufman (ME/cfs specialists in California) and — this is the part for anyone who might be overwhelmed with where to start — a local naturopath (ND). In fact, the best help I got in Seattle was from two different NDs: they thought outside of the box and dug a little deeper, like the specialists. And I don’t mean woowoo shit, I mean things like checking for an immune deficiency DUH since I keep telling you it feels like my immune system just broke one day. Soon after I traveled to California to see Dr. Chia, I found an ND who ran almost the same battery of tests which revealed the same abnormal results. The first ND, who agreed I needed IVIG, but couldn’t get it for me, tried a bag of different tricks aimed at increasing my IgG levels. They didn’t work, but I was very grateful to have someone try something. Point being, if you can’t see a specialist, I would advise finding an ND who will look at your immune system health and infections and who is willing to walk the long road with you, being patient while you try (and, in my case, most often fail) different treatments.
But, I got ahead of myself. Dr. Chia saw that my total IgG was low and so were some of the IgG subclasses. He said I needed IVIG, but he didn’t offer to get it for me (I thought at the time it was because he was in California, but I now know Seattle patients that get IVIG through Cali doctors, so I’m not sure why he couldn’t have ordered it). Once I was back home, I asked my 4 doctors if they could help me get IVIG (primary care doctor, rheumatologist, endocrinologist, ND) and they all said no. My PCP did go a little further by asking an immunologist colleague, but he said my IgG would need to be lower or I’d have to do a vaccine challenge, which I refused.
I had given up and stopped asking when I found my second ND (who was very different from my first; both have been helpful in separate ways). The very first thing she said after entering the room on our first meeting was: “You need IVIG.” She had reviewed my lab work (she had reviewed my lab work!! I don’t think any other doctors had actually looked at anything ahead of time) and seen that my IgG was continuing to decrease over the months. I had hypogammaglobulinemia and fit the diagnosis for common variable immune deficiency (CVID) and she was confident insurance would approve immune globulin therapy.
Between that day and my first infusion, 11 months went by. I delayed until I felt I had thoroughly prepared in every way to keep myself safe. Anaphylactic or anaphylactoid reactions can occur in any patient receiving IVIG therapy, but I had a history of both (plus intractable migraines), so I was nervous and wanted to control every aspect of treatment. My doctor was patient and accommodating. I don’t think any other doctor would have let me take the time to tackle each concern and build up the confidence to take the plunge. I think of it a little like a lost year when I could have been feeling better, but, like I said, I really can’t have regrets when things went so well.
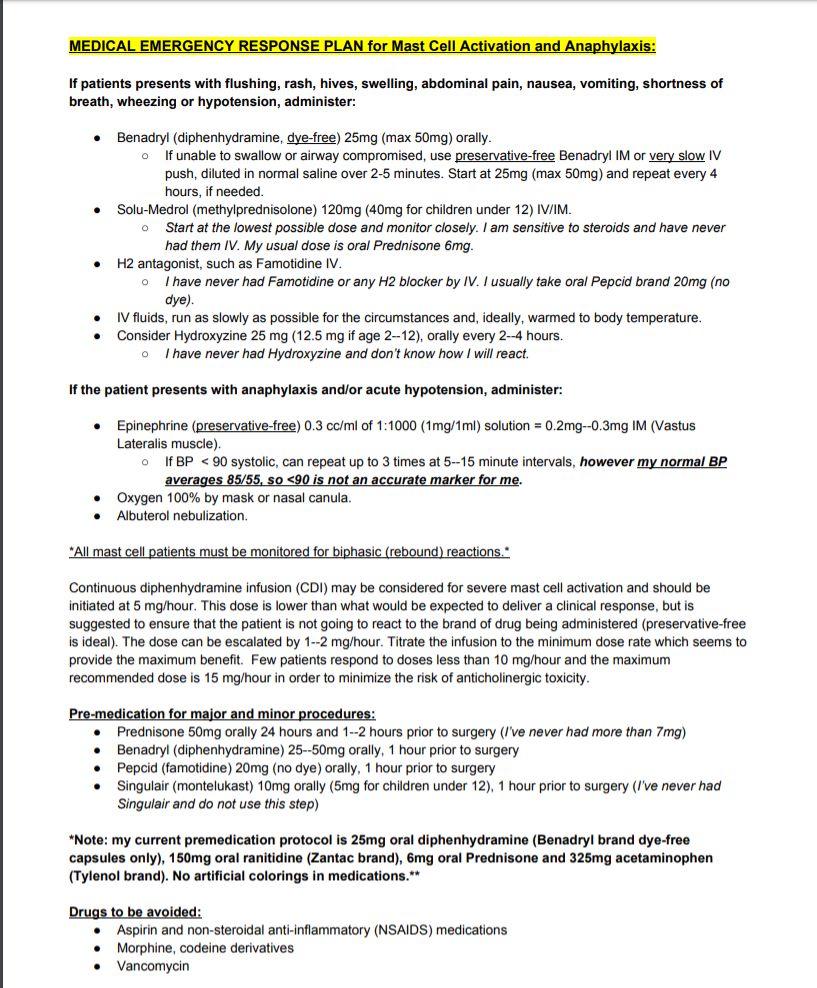
First off was figuring out how to safely take pre-medications for potential reactions to the immunoglobulin and how to get IV fluids (which would be administered before IVIG) without side effects. I was extremely reactive back then because of out-of-control mast cells and I had no safe rescue medications or pre-medication protocol. IV fluids had caused angioedema and breathing issues; I was so sensitive to Benadryl, I couldn’t even take drops without feeling anticholinergic-type symptoms; tiny crumbs of steroids made me feel like was hit by a truck, running on a treadmill and sedated all at once. I didn’t feel comfortable doing IVIG without having a rescue protocol, so, during that year, I worked on my tolerance and put together a safe plan.
First, my doctor put me on bioidentical hormones because there is some evidence that they can help with mast cell reactivity. Then, we tried IV fluids, but only 250 mls, warmed up and run at a snail’s pace (my previous reactions were from 2,000 mls of cold fluids run very quickly on the day my period was due (when I’m highly reactive); I didn’t know any better). I even found out I was fine with two types of normal saline bags, but not another. I slowly gained tolerance to Benadryl (dye-free capsules, only) and Prednisone (finding manufacturers with the cleanest excipients), taking bigger and bigger slivers until I knew I could safely premedicate before infusions. Those that know me understand that the symptoms that have scarred me the most are my mast cell reactions. They are unpredictable and violent. Full-blown anaphylaxis almost killed me. I can’t adequately express how jubilant I was to have a safety net, to have protection, to be able to put a protocol on paper that anybody could follow in case of an emergency and to have tools with which to arm myself before a procedure. Having intolerable side effects from the things that are meant to counteract intolerable side effects was a scary place to be.
Next, I talked to my doctor about starting with subcutaneous infusions (SCIG), rather than intravenous because all of my research indicated that the former was safer. She agreed, thankfully, although she gently pushed for IV for years after that. I also asked if I could start with 1 gram at a very slow rate of delivery and she acquiesced to that, too. NO allopathic immunologist would have agreed to that EVER.
Then I looked into a hospital infusion versus an ambulatory infusion suite (AIS) versus at-home infusions. I was told a hospital wasn’t an option and the AIS was staffed only with a nurse, no physician. If I had a reaction, the protocol was for the nurse to administer supportive meds and call 911, if needed. Well, staying at home was a no-brainer. I would have a nurse in my house, but, more importantly, I feel much safer with my husband there as an advocate. Plus, we live very close to an emergency room and he could whisk me there if calling an ambulance didn’t feel like the appropriate move. In the past, we have sat in our car in the ER parking lot, waiting to see how reactions progressed. The high price of healthcare in this country is a great deterrent.
Then I wanted to look into IgA deficiency. There is some research that low serum IgA and anti-IgA antibodies increase the risk of anaphylaxis and the remedy would be to use a very low-IgA brand of immune globulin for my infusion (says my Labcorp test result: “Patients with IgG antibodies against IgA may suffer from anaphylactoid reactions when given IVIG that contains small quantities of IgA. In one study (Clinical Immunology 2007;122:156) five out of eight patients with IgG anti-IgA antibodies developed anaphylactoid reactions when IVIG was administered.”). My total IgA and one IgA subclass had been low in the past, but neither my doctor nor the infusion pharmacist suggested that this should be a consideration — I had to get the info from other patients and insist (nicely) that we test my anti-IgA antibodies. Gamunex-C was the brand that had already been approved by insurance and I knew that I was very lucky to have it and might lose it if we had to resubmit an authorisation, but safety first. Gammagard could have been a safer choice since it has extremely low IgA content. It took an excruciatingly long time to get those results but, ultimately, I did not show anti-IgA antibodies, so we pressed ahead with Gamunex. And I’m glad we did! One of my nurses commented that it is the “top shelf” immune globulin and it’s been good to me.
The final hurdle was scheduling. Back then, I was much sicker in the mornings — shaky and very low blood pressure — but that is the time of day when nurses typically arrive for long appointments. I always thought, if I became a home infusion nurse, I would offer nights and weekends, just like my preferred shifts in the restaurants. There must be more patients like I am whose vitals stabilize as the day goes on. Also, my period was looming, a time of the month when I am highly reactive, so I wanted to avoid that whole week (although this wasn’t as easy as it sounds because my cycle wasn’t/isn’t regular). The day came when things eventually fell into place and my wonderful nurse, Marie, came to my house to hook up the IV fluids and teach me how to infuse subcutaneously. She showered beforehand and changed her clothes because she and some of her other patients have cats. She understood my nervousness and didn’t rush me or complain even though she had to sit in one room with me in a straight-backed chair for 8 hours. Marie came every week for 16 months to hook up my IV, but, once we knew I was doing well on this treatment, she was able to leave quickly and I would disconnect my IV fluids and do the SCIG myself.
We started with 1 gram infused through a 2-needle set and F30 tubing. That probably made anyone knowledgeable with immunoglobulin infusions laugh because it is SO SLOW. Like, unheard of. My nurse had to do a special order for the supplies because they are normally only used for infants. Over the weeks, we slowly worked up to 5 grams (eventually using a 3-needle set and F45 tubing — only slightly faster), which is a typical ‘replacement’ dose for a primary immune deficiency patient of my weight. I stayed there for a year and a half, not pushing my luck in any way. Slow and steady.
In 2017, a miracle: I switched infusion companies from Coram to Accredo (with nothing to which to compare Coram, I thought they were fine, but things have been much better with Accredo) and they suggested I learn to insert my own IV catheter for fluids. Uuh, yes, please! Actually, they suggested my husband do it, but he’s not good at these things and I am, so a nurse came over and gave me a tutorial and that was that. I was only “allowed” one training session, so I wound up watching a ton of YouTube videos, which is why I’ve now made my own, in case they can be helpful for anyone.
For over 3 years, I’ve been placing my own peripheral IVs each week. It gets easier and easier and, honestly, I feel so much safer. Although Marie was very careful, I am more careful because I have a bigger stake in the game. I do not want to ruin any veins or get an infection, so I am vigilant (and superstitious) about my aseptic technique and I rotate veins to give them a break. Every single week, for the entire 16 months that Marie was my nurse, she used the left median cubital vein (antecubital or, as my nurses called it, the “AC vein”). I never questioned it because it held up well, but that’s about 60 catheters inserted in the same place (what a trooper my vein was!). As soon as I was doing it myself (and discovered I was ambidextrous when it comes to IV placement), I started using a different vein each week. I have 6 sites that I use, but 2 of them (on the outside of my forearms) are difficult — the veins roll and there’s always more of a risk of having to do multiple pokes — so I use the cephalic and AC veins more often than not, even though it means having to keep my arm straighter. I don’t use my hands or wrists, partly because I wash my hands so often, it’s an inconvenience and partly because I want to save those sites for easy access if I’m ever in the hospital with a nurse that needs fat veins for larger gauge needles.
Holy roller
Then in 2018, another miracle: I switched from SCIG to IVIG and was able to continue to do it myself at home. Not only that, but I was allowed to continue infusing once a week, which kept my levels more consistent with fewer peaks and troughs, which in turn kept my energy more stable. IVIG is typically given every 3 or 4 weeks for multiple days in a row, necessitating a peripheral IV be left in place for 3 or 4 days (I can’t even imagine; 12 hours feels like an eternity). This is one of the reasons so many people get PICCs or ports.
I am regularly asked how I managed to get self-infusion approved at home. I didn’t do anything. I didn’t even know it was something that was allowed. I lucked into it with a good doctor, a good infusion company and a good nurse.
The first year I was with Accredo, I had increased my SCIG dose from 5 grams to 10 grams. My legs (my preferred place for the subcutaneous needles) weren’t happy, though. They weren’t absorbing the medication as well as they used to and they were swollen and sore for longer afterwards. I was using 6-needle sets to try to stop leaking and I felt like a pin cushion. I also wanted the option of trying high-dose IgG (my specialist had said for years that I needed 20 grams/week) in the remote chance that insurance would approve it. So I talked to my doctor about changing brands to one with a higher concentration, which would mean less fluid infused into my tissue. I was still adamant that I didn’t want to try IVIG. I didn’t want to tempt fate and I was scared of medications going directly into my veins and causing an instant reaction. My doctor pointed out that my body liked Gamunex, so I could either stick with what we knew didn’t cause a reaction (because Gamunex can be infused by either route) or stick with SCIG and change brands. I decided that it felt safer to stick with the brand I knew and loved, so IVIG it was.
They sent a home health nurse to do the first IVIG infusion. I had already placed my IV catheter and run my fluids when she arrived and she said it was perfect. Once again, we started at a low dose (2.5 grams) and ran it very slowly. We worked back up to 10 grams a week over a few months. During this time, I changed from the first awful, bullying nurse to one I adored (we could be friends in a different life). Jennifer showed me how to run the IVIG after the fluids and made sure I did everything right, but one week she said, “I’m just a fly on the wall. You place the IV, you run the fluids and medication, you disconnect. There’s no point in my being here.” So she recommended to my doctor that I do it alone under the condition that I have a responsible adult available at all times during an infusion in the case of anaphylaxis. That’s how I wound up doing it without a nurse and I’ve never met anyone else who is in this same situation.
The final miracle happened this year: My insurance approved the high dose IVIG (20 grams a week, which works out to almost 2g/kg/month, what is considered autoimmune or immunomodulatory dosing). I’m not sure which of my ridiculously high titers got it authorised and I’m not going to question it, I just thank the universe each week and try to keep finding the money (my 20% copay is $1,400/month). I increased slowly over months and had some headaches in the beginning, but nothing now. I am energised the day after. It’s like liquid life-force. I only premedicate with 25mg Benadryl, 20mg Pepcid and 4mg of Prednisone and I could probably do less. The number one benefit to doing it solo is that I’m able to program the flow rate as slowly as I like, which ameliorates side effects. If I had medical oversight, I’m sure they would insist I increase the rate, if for no other reason than to get the nurse out of here quicker. Talking to friends who have dealt with aseptic meningitis or incapacitating migraines, it seems to me that flow rate being too high is the major precipitating factor.
IVIG changed my life. I started the first wee tiny dose on October 2nd, 2015 and improvements in ME symptoms happened very quickly. By January 2016, I felt confident enough to write about them. They marked the end of 4 years of a steep and terrifying downhill trajectory and the beginning of a very slow, but steady uphill trajectory for the past 5 years. There have been lots of setbacks, plateaus and crashes (scary ones and months-long), but, overall, I’m stronger and more able-bodied each year over the last.
There are so many things I’ve learned along the way that I want to share like: try to get shelf-stable bags of fluids. My first pharmacy removed the air from the bags of saline before sending them and I didn’t know that there was another option. Once the bags have been accessed to remove air, they have to be refrigerated and thrown out after 14 days. They take up a lot of room in the fridge, it take ages for them to come to room (or body) temperature and you can’t have extras on hand when they’re considered unsafe after a few weeks. My bags now can be stored at room temperature in my closet and their expiration dates are years away, which means I have them for emergencies and don’t need to go to the hospital if all I think they can do for me is administer fluids (which is what has happened so many times in the past with my vasovagal collapses).
This took on even greater importance when covid hit. I feel so lucky to have extra supplies and the ability to give myself IV fluids without going near healthcare facilities. When I’m doing the clean-out for an upcoming colonoscopy, my doctor wants me to give myself IV fluids, which I wouldn’t have been able to do without this lucky situation. And when I imagine the big earthquake or an end-of-world emergency, it gives me solace to know that I am trained and my home is so well equipped.
I’ve also learned that I never want to use gravity tubing and an IV pole when a pump and carrier bag is so much easier, safer and more precise. I don’t have to keep my fluids vertical and elevated, dragging a pole around the house; I can walk around with the bag holding the saline and pump on my shoulder like a purse. I’ve even gone to doctor appointments and run fluids in the car during our California road trip last year after a big blood draw.
I learned from other patients to prime the air out of the bags through the tubing before priming the saline (fill the tubing with saline), which seemed slightly safer than the way a nurse showed me using a syringe, which requires accessing the rubber stopper. Uses fewer supplies, too. Less plastic waste.
Medical waste
I called B. Braun, the company that makes my normal saline, and learned how to safely warm the bags before administration, so I don’t react to the room temperature (which is chilly!) fluids. I figured out that running fluids at a slower rate (150ml/hour) cut down on post-infusion headaches and it was even more effective to bookend the Gamunex with 500ml of saline before and after, rather than running the entire liter beforehand.
I learned that I can keep using the pump for 12 hours after it beeps that the battery is low. Again, less waste. (Although, I wouldn’t sleep with a low battery, just in case.) And I learned that the Bodyguard pump’s beeps terrified my dogs because they were too similar to our fire detector, but the CADD Prism’s beeps go unnoticed.
Bad beeper
Wonderful nurse Jennifer gave me a fabric one-handed tourniquet which has made such a difference to my independence and the comfort of my skin. She also taught me that if the ultrasite on the saline lock is going to be unattached for any length of time and I don’t have a cap for it, an old nursing trick is to stick it inside an alcohol prep pad (leaving the wrapper on) and secure it with tape.
Wonderful nurse Marie taught me how to use gauze to support the catheter if it doesn’t lie flush with the skin and how to tape a loop of tubing to your arm, which has stopped my IV from being yanked out many times when I snag it on something. She also always used alcohol prep pads and iodine to clean the insertion site, something which many find overkill, but makes me feel more confident in my infection control.
I learned the catheters with wings are much easier for me to insert than the ones without and that you can ask for sterile gloves rather than relying on the box of non-sterile gloves that they send by default. I learned that you can order sterile pads on which to lay your supplies and IV3000 adhesive dressing that doesn’t tear up your skin like the Tegaderm that comes inside IV start kits.
I figured out by trial and error that some veins need to be stretched taut and stabilised and, if you are inserting your own IV and don’t have two hands, there are ways to do this by twisting your forearm and flexing your hand. I also found out that some veins are close to nerves and your thumb might have pins and needles for weeks afterwards, but they will, thankfully, eventually go away.
During SCIG, I learned that there are handy rate and time calculators for subcutaneous infusions and that if you are having trouble with leaking, swelling, hitting blood vessels etc., that you can try different needle lengths and different needle brands and — the key for me for whatever reason — different needle tops (the soft adhesive ones worked best for me rather than the hard plastic ones that needed to be covered with Tegaderm). I also learned that fat is key to comfort — the medication was much better absorbed if I put the needles in the back of my hips/ top of my butt (saddlebags??).
The most important thing I’ve learned is that although most patients in online support groups ARE NOT MEDICAL PROFESSIONALS AND YOU SHOULD ALWAYS CONSULT YOUR DOCTOR ABOUT EVERYTHING, they are a wealth of information. Doctors and pharmacies didn’t tell me anything about how to manage infusions safely. The majority of my home health care nurses didn’t verbally educate me — it was up to me to observe, ask questions and do my research.
I’m going through a rough(er) patch. My body is scaring me because I can’t find any cause for recent episodes. One of the good things these past few years, is that I can usually pinpoint a reason for reactions and downturns. Even after the last horrific night I suffered with apparently no reason (it was last November, during my Dad’s very short visit and I couldn’t blame it on overdoing it because I didn’t), I started spotting late the next day and–light bulb!–it was my period coming a week early (I can have terrible reactions on the day before or the first day of menstruation).
When my husband called 911 on the first day of my last period (both my MD and ND said that my body had gone into shock), it was the first time I’d had such a bad collapse with vitals bottoming out since 2010 — since before I was sick! Then, 5 days later, I got a tingly tongue and lip during IVIG and then a hive on the base of my throat. I realise it was a tiny reaction compared to what so many mast cell patients go through (a week later, a friend of mine went into full-blown anaphylaxis during her IVIG infusion and then somehow got the guts to try again the next day with the same batch –that put my experience into perspective), but the thing is, except for one small hive when I tried Xanax in 2013, I hadn’t had any hives since being in full-blown anaphylaxis 17 years ago! And that place–a hive in the suprasternal notch– was always the position for a systemic red alert, for something I ingested, as opposed to benign contact dermatitis.
Then Saturday evening, my tongue swelled up for the first time in 7 months for no reason that I can figure out. I had tongue swelling a few times last year, but I could always explain it (dental work, sauna, vancomycin). Even more concerning, it’s still swollen now, 45 hours later and that’s very unusual. I took Benadryl the last 2 nights, squirting it onto the affected area of my tongue, as I’ve been told to do (this is also unusual for me–I am extremely judicious with Benadryl, only taking it when absolutely necessary) and the swelling still hasn’t resolved. I can’t remember another time it lasted this long — maybe, again, 17 years ago during anaphylaxis.
Then yesterday afternoon, I was hit with vertigo after spending too much time on my feet, preparing food. Vertigo is rare for me and is a big red flag. It’s very different from dizziness and I don’t think it has anything to do with blood pressure. I went to bed for a while, hoping it would resolve, but, when I got up, I was still slamming into walls, as if I were walking the hallway on a lurching boat. The last 2 times I experienced vertigo were 5 months ago during–shocker–my period and a year ago on the morning we were leaving for California, after killing myself the day before to finish packing. I thought it might be something to do with my neck, which always has issues, so I used heat, then my cervical traction device, then an ice pack. I think it helped; the vertigo had mostly abated by the time I went to bed.
But…
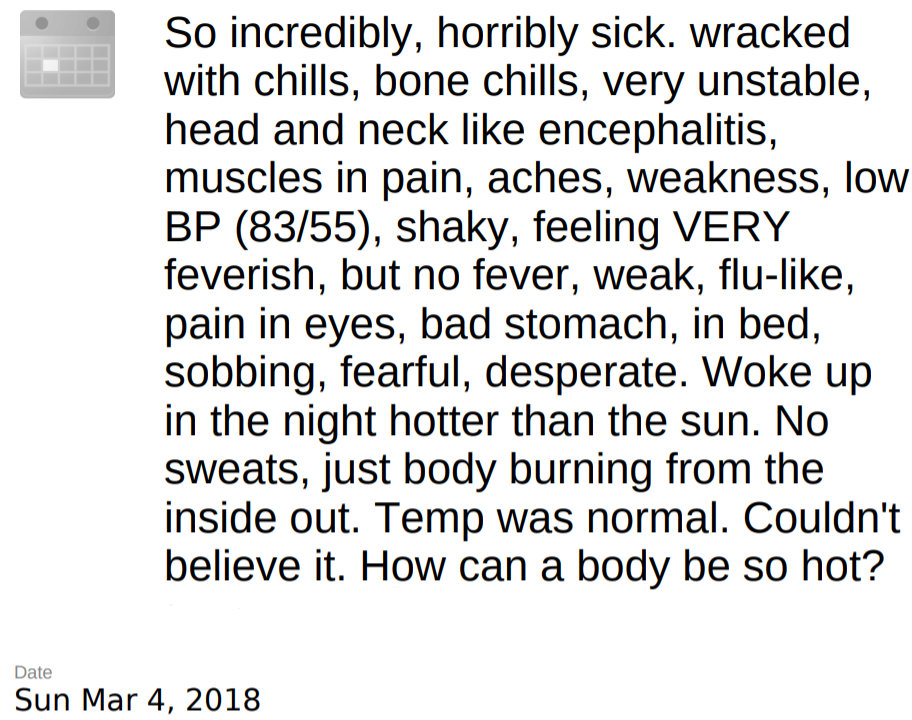
A few hours after I went to sleep, I woke up with horrible shakes and chills and drenching sweats. My BP was low (but low-normal for me: 80/50), HR was a little high, temperature was 96 degrees, and O2 was 95%. It was 7 terrible hours that felt viral, like when I first got sick, but was probably mast cells, what with the swollen tongue and all. I finally got up to do that thing that other chronically ill people might understand: put on clothes in case I had to go to the hospital. On a normal day, I might sit around in my dressing gown with unbrushed hair all day, but when there could be a chance I’m going to the hospital, I try to make sure I’m not naked. I also make sure I’m not wearing anything I care about — I’ve lost clothes in the hospital before.
Strangely, I had almost an identical episode on this exact day last year. Here’s a screenshot from my calendar:
After the most stable autumn and winter I’ve had since being sick, this downturn–this piling on of relatively rare, red-flag symptoms–scares me. My sleep has gone to hell in the last few weeks, which compounds everything by stealing energy and increasing pain. Plus, I’m exacerbating things by holding tight to my “best winter yet” narrative and by fighting so hard to maintain the level of functioning I’ve had this past year, rather than pulling way back and resting aggressively.
My ND says the naturopathic philosophy is that you will go back through previous stages of health and experience earlier symptoms as you travel the healing journey back to where you once were. I’ve latched onto this theory to anchor myself and dispel some fear. The resurgence of all these old symptoms means there has been a shift in my system — but maybe it’s a positive shift, even though it doesn’t feel that way. I’ve gained weight since starting IVIG, over 8% of my norm, which is not insignificant, especially on someone as small as I am. I’m at my heaviest since being sick and, although I’m not overweight, I’ve lost muscle tone the last 7 years and I don’t have the physical ability to burn fat and build muscle, so I hope this trajectory doesn’t continue. My doctor thought this, also, pointed towards a shift in my body: maybe I’ve started absorbing nutrients better. Acne is coming back a little, too. Maybe my hair will grow back! Or the next thing will be that I’ll catch a cold for the first time in 8 years… (And because I really don’t want this to happen, no matter what it might indicate about a calming immune system: knock on wood, toba, toba, spit over shoulder: patuey.)
But, as I lie here, shaky, with my swollen tongue, chronicling these last few weeks (minus the osteoporosis diagnosis and extremely elevated post-antibiotics SIBO test results, both of which I’ll have to write about at a different time), none of it feels like a positive shift and I worry about what I should eat so as not to add to mast cell reactivity and whether I should stay in bed and lie still, even though longed-for Seattle sun is streaming through the windows and I’d love to make some breakfast and sit at my table watching Riley lounge in the grass, soaking up the rays, and the hummingbirds diving around our feeders.
SALT LAKE CITY, UT — Mast cell activation syndrome (MCAS) may be an overlooked yet potentially treatable contributor to the symptoms of chronic fatigue syndrome/myalgic encephalomyelitis (ME/CFS), say physicians who specialize in ME/CFS and its manifestations.
The subject was discussed during a 2-day clinician summit held March 2 to 3, 2018, during which 13 panelists met to begin developing expert consensus guidance for primary care and specialist physicians for the management of the complex multisystem illness ME/CFS, and to recommend research priorities.
“ME/CFS is a descriptive diagnosis of a bunch of symptoms, but it says nothing about what’s causing the symptoms, which is probably part of the reason it’s so hard for it to get recognition. So, the question becomes, What other pathology is driving this illness and making the person feel so ill? I think mast cell activation is one of those drivers, whether cause, effect, or perpetuator, I don’t know,” internist David Kaufman, MD, who practices in Mountain View, California, told Medscape Medical News.
MCAS is a recently described collection of signs and symptoms involving several different organ systems, that, as with ME/CFS itself, do not typically cause abnormalities in routine laboratory or radiologic testing. Proposed diagnostic criteria were published in 2010 in the Journal of Allergy and Clinical Immunology.
Kaufman first learned about MCAS about 5 years ago from a patient who introduced him to the published work of mast cell expert Lawrence Afrin, MD. “I spoke to him and then I started looking for it, and the more I looked, the more I found it,” Kaufman said, estimating that he has identified MCAS in roughly half his patients who meet ME/CFS criteria.
Indeed, summit panel member Charles W. Lapp, MD, who recently retired from his ME/CFS and fibromyalgia practice in Charlotte, North Carolina, told Medscape Medical News, “I see a lot of this. I think it’s one of the many overlap syndromes that we’ve been missing for years.”
Another panel member, New York City ME/CFS specialist Susan M. Levine, MD, also said she sees MCAS frequently. “I suspect 50% to 60% of ME/CFS patients have it. It’s a very new concept.”
In Levine’s experience, MCAS often manifests in patients being unable to tolerate certain foods or medications. “If we can reduce the mast cell problem, we can facilitate taking other drugs to treat ME/CFS,” she said. However, she also cautioned, “It’s going to be a subset, not all ME/CFS patients.”
Clinical Assessment and Laboratory Testing
As discussed at the summit, for patients who meet ME/CFS criteria, the next step is to drill down into individual patients’ symptoms and address treatable abnormalities. Investigation for MCAS may yield such findings among those who exhibit episodic symptoms consistent with mast cell mediator release affecting two or more of the following areas:
Symptoms can wax and wane over years and range from mild to severe/debilitating. It is important to ask about triggers, Kaufman advised. “The patient is usually aware of what makes them feel worse.”
Routine laboratory assessments include complete blood count with differential, complete metabolic panel, magnesium, and prothrombin time/partial thromboplastin time.
More specific laboratory testing can be tricky, as the samples must be kept cold. These include serum tryptase, chromogranin A, plasma prostaglandin D2, histamine, heparin, a variety of random and 24-hour urinary prostaglandins, and urinary leukotriene E4.
For patients who have had a prior biopsy, the saved sample can be stained for mast cells.
Kaufman said that initially after he learned about MCAS, he would only run the laboratory tests in patients with suggestive clinical history, such as food sensitivities/triggers, rashes, hives, temperature intolerance, or chemical sensitivities. “But ultimately, I had patients [for whom] I couldn’t figure out what was going on; I would check, and started finding positives in patients I wasn’t suspicious of.”
So, now he just tests for it in all his patients with ME/CFS. “It’s bigger than allergy,” he remarked.
Treatment May Ease Some ME/CFS Symptoms
Treatment of MCAS involves trigger avoidance as possible; H1 receptor antagonists such as loratadine, cetirizine, or fexofenadine (up to double the usual doses); H2 histamine receptor antagonists including famotidine or ranitidine; and mast cell membrane-stabilizers such as cromolyn sodium. Slow-release vitamin C can also help in inhibiting mast cells.
Over-the-counter plant flavonoids such as quercetin also may be helpful, typically at high doses (up to 1000 mg three times daily). “There’s a long list of medications that either quiet down mast cell activation or block the receptor,” Kaufman noted.
But despite that, without controlled trials, it is difficult to determine the exact clinical effects of blocking mast cells, especially as these patients tend to be taking many other medications. And in the context of ME/CFS, the extent to which suppressing mast cell activity addresses the core symptoms of fatigue, postexertional malaise, orthostatic intolerance, and cognitive dysfunction is unclear.
Kaufman noted, “I think treatment clearly helps with the fatigue because they’re not reacting to everything. It improves gastrointestinal symptoms, so they can eat better…. I have seen [postural orthostatic tachycardia syndrome] improve, but I have to say I also give meds for dysautonomia, so I can’t be sure.”
Lapp said that in his experience, “[Patients with ME/CFS] aren’t cured, but do get better. [Blocking mast cell activity] gets rid of dizziness, fatigue, nausea, and light sensitivity.”
Levine pointed out, “We’re just at the beginning of identifying this patient subset and thinking what makes sense to try…. One thing that’s sure is that the drugs are pretty safe,” she said, adding that when it comes to working up patients with ME/CFS for MCAS, “There only seem to be good things that can happen.”