A DECADE
A decade since I felt well.
A decade since my body and health were not on my mind.
A decade since my last cold, flu or bronchitis.
A decade since my last vaccination.
A decade since I enjoyed Halloween, my favourite holiday.
A decade since I was in a lake or ocean.
A decade since I was on a train.
A decade since I stood up at a concert.
A decade since I didn’t wear a mask on a plane.
A decade since I went to a wedding.
A decade since I went to a barbecue.
A decade since seeing so many friends.
A decade since I married my longtime boyfriend because “I feel like something is going to happen to me and I want you to be able to legally speak for me, if I can’t speak for myself.”
A decade since I was in Ireland, in my childhood home, walking the streets of my heart.
I thought about this anniversary so many times in the past. For a long time, I thought there was no way it would come–I couldn’t possibly stay sick this long. Every other illness had a beginning and an end, so, surely, one day my body would recover and this spectre would leave, it was just taking a little longer than the usual virus.
Once I realised it was lifelong, I thought the 10-year mark would be a momentous and heavy occasion. It turns out, it’s not. 2 years seemed much harder to accept. Back when isolation was still harrowing and loneliness still suffocated. You get used to both. It helps if you can develop a deep disdain for humans, so you can trick yourself into believing you’re not missing out on anything. And the 5-year mark was hard. I’d felt small, but miraculous changes from IVIG and then had an epic autumn backslide that year. The dowsing of that little flame of hope was devastating and it was inconceivable that I would be physically or mentally resilient enough to continue the maybe-I’m-getting-better!-Oh-no-what-fresh-hell-is-this? cycle for years to come.
But, then, suddenly, 10 years have passed. I could almost believe the rest of the world is trapped in amber, frozen in time, awaiting my return. As soon as I kick this thing, I’ll drive back down to the office–each street scene melting and returning into motion as my car passes by–and get back to work. Thanks for waiting, guys.
INFECTIONS
What’s far more unbelievable to me is that I haven’t had a muggle illness in a decade. [Please don’t let this jinx me.] No head cold, no flu, no stomach bug, no chest/ear/sinus/bladder/any-other-part-of-the-body infection. The more time that went by, the more ominous was the thought of contracting an acute virus. For years, I had relentless flu-y symptoms–headaches, sore throats, muscle pain, weakness, chills (and still do, sporadically)–and I have many high out-of-range infection titers*, so the thought of another malady compounding the daily slog was harrowing.
*HHV6 IgG; HSV IgM; EBV IgG; M Pneumoniae IgG; S. Cerevisiae IgG; Varicella IgG and IgM; Coxsackie A7, A9, A16, A24, B1, B2, B5 and B6; Anti Streptolysin O Titer, and Candida IgM and IgA. Yes, really.
Three years into my illness, Dr. Chia told us unequivocally that a run-of-the-mill cold could make me permanently worse, so we have always taken great precautions to avoid exposure, which have only intensified during this pandemic. I honestly wonder if I’ll ever be indoors and maskless with anyone besides my husband again. Even worse, will my husband ever be indoors and maskless with anyone besides me? It’s one thing to choose this life for myself–I’ve made peace with only having remote communication with friends and family; I have a partner and a dog to keep me sane–but my healthy husband’s life has shriveled to keep me safe and the guilt from that is indescribable. I imagine if he weren’t yoked to someone at such risk for serious complications from viruses, he might be out gallivanting and socialising, as well he should be.
VACCINES
One of the first doctors I saw after falling ill said, “You are very sick. We don’t know what’s wrong with you, but you should never get another vaccination as long as you live.” I was confused because, until that moment, I hadn’t linked whatever this sickness was to the flu shot I’d gotten a week before Halloween. I was also confused because, in my healthy ignorance, I thought vaccines only bolstered your immune system. I really didn’t understand, in certain unique circumstances, that they could break it. I used to get every immunization available in an effort to protect myself.
Before I traveled to Central America, I was vaccinated for polio, live typhoid, hepatitis A and B, tetanus, diphtheria and gammastan–all on the same day. In the years after, I got the live varicella vaccine, the 3-shot hepatitis B series, measles, mumps, and rubella and, of course, the flu shot every year, along with a pandemic flu vaccine (H1N1) when they were offered. I didn’t get majorly sick while traveling, I didn’t get chicken pox when I tended to my horrifically poxy husband and I never got the flu despite working very long hours in restaurants, among infectious people (note to the public: restaurant staff work when they’re sick; you have to be on death’s door to ask someone to cover a shift), so I guess the vaccines helped… until they harmed.
COVID
There’s such polarization these days when it comes to covid vaccines. There’s a lot of hatred directed at those who are trying to protect themselves and others by getting vaccinated and wearing masks and there is an equal amount of contempt directed at anti-vaxers. I have yet to see a single news story talk about those of us who want to get vaccinated, but cannot. Or those of us who have to make the agonizing decision to live a life of extreme isolation or risk very serious repercussions from a vaccine–any vaccine. I wish individuals would always take the collective into consideration and try to protect those that are vulnerable, but that’s not human nature, unfortunately. People will refuse vaccinations or not wear masks or not get tested because they don’t want to quarantine. And, all the while, those of us with weakened, damaged or overactive immune systems–be it from chemo or old age or autoimmunity or ME/cfs or steroids or stress or another condition–will have to choose seclusion over risk.
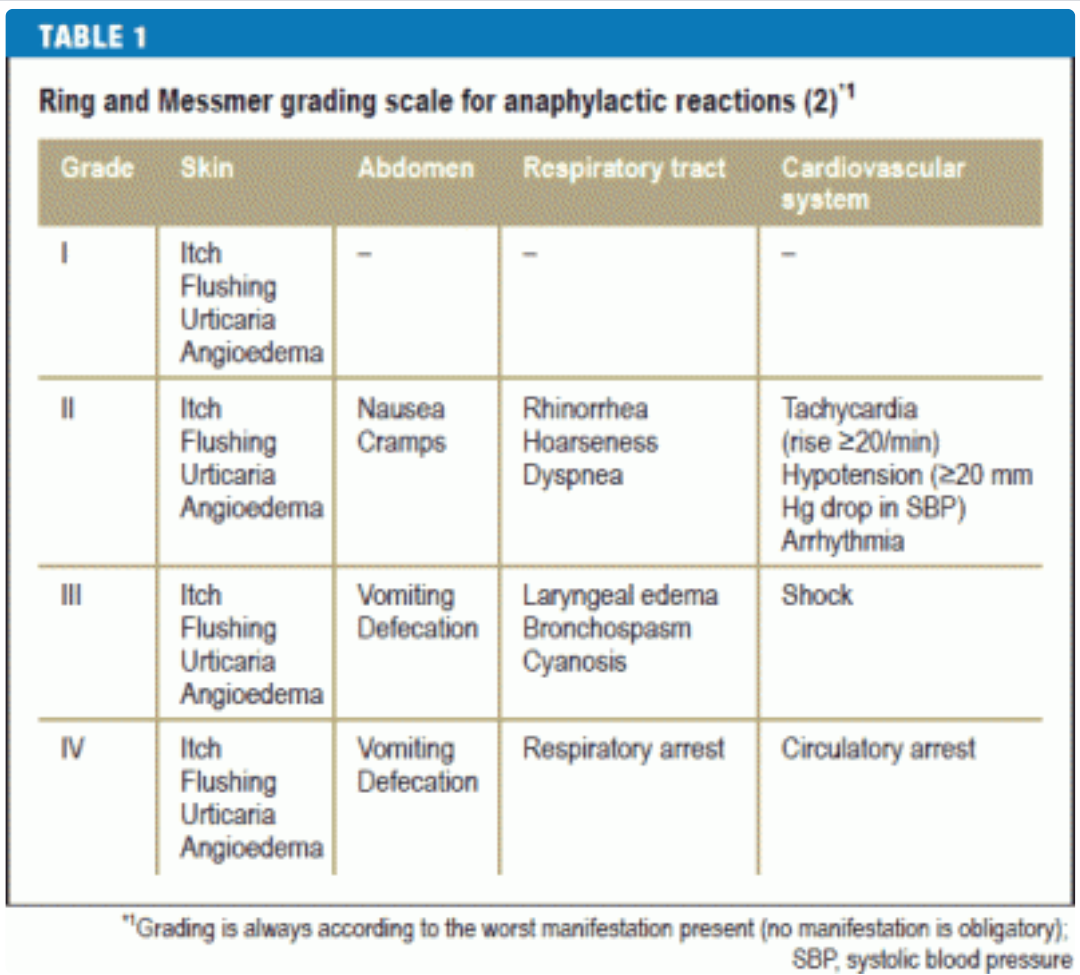
Against one of my doctor’s advice, I will be getting the first covid vaccine next month–but I’m getting a pediatric dose. We will see how I do and then I’ll get a second dose and test antibodies. They will be keeping me for observation in the clinic for an hour because of my history of anaphylaxis, but that’s not what I’m worried about.
I’m worried about being bedbound again. I’m worried about volunteering for an injection that could further damage my autonomic nervous system and intensify dysautonomia and hyperadrenergic symptoms. I’m worried about triggering more vasovagal collapses or making myself more hemodynamically unstable. I’m worried about a cytokine storm and/or a mast cell meltdown that creates a permanent worsening of reactivity when I’m already so limited in medication options and trying so hard to keep on weight. I’m worried about a blood clot causing sudden death because IVIG, oral hormones and inactivity already put me in a high-risk category. I’m worried about losing the limited amount of independence and mobility I have now (but it’s enough for a happy life) and becoming too weak to even wash my hair again. I’m worried about being that burden to my husband again, especially now that it takes so much work to make my GI tract function–it would be a monstrous task for him to take on. Mostly, I’m worried about once again losing the small joys, like taking Penny on our scooter walks, being able to talk on the phone for hours and laughing. I spent years without those gifts and I’m not sure I can claw my way back over another decade.
It feels good to write out those fears. There are very few people with whom I can have these discussions because not many healthy friends understand the risks involved when dealing with such complex conditions. Everyone in my family has had at least 2 covid vaccinations with no side effects, but, in my support groups, it’s a different story. Even there, though, I am careful–I want everyone to get vaccinated, if they can safely, and I never want to dissuade others by voicing my concerns. And doctors aren’t much help because the vast majority take the practical stance that, statistically, the chances of negative repercussions are low and that the risks outweigh the benefits. That’s absolutely true for the typical bell curve of the typical population. Not true for me.
Let’s just hope it’s all smooth sailing. I’d like the next decade to be different.
Update: My doctor pretty much talked me out of getting the C vaccine. I’m too high-risk for long-term reactions. I’m going to have to get surgery next year, so not being vaccinated in a hospital setting adds another layer of fear, but I won’t be stable enough for surgery if the vaccine caused damage. So I will be remaining in strict isolation and putting my life in other people’s hands.