A decade since my body and health were not on my mind.
A decade since my last cold, flu or bronchitis.
A decade since my last vaccination.
A decade since I enjoyed Halloween, my favourite holiday.
A decade since I was in a lake or ocean.
A decade since I was on a train.
A decade since I stood up at a concert.
A decade since I didn’t wear a mask on a plane.
A decade since I went to a wedding.
A decade since I went to a barbecue.
A decade since seeing so many friends.
A decade since I married my longtime boyfriend because “I feel like something is going to happen to me and I want you to be able to legally speak for me, if I can’t speak for myself.”
A decade since I was in Ireland, in my childhood home, walking the streets of my heart.
I thought about this anniversary so many times in the past. For a long time, I thought there was no way it would come–I couldn’t possibly stay sick this long. Every other illness had a beginning and an end, so, surely, one day my body would recover and this spectre would leave, it was just taking a little longer than the usual virus.
Once I realised it was lifelong, I thought the 10-year mark would be a momentous and heavy occasion. It turns out, it’s not. 2 years seemed much harder to accept. Back when isolation was still harrowing and loneliness still suffocated. You get used to both. It helps if you can develop a deep disdain for humans, so you can trick yourself into believing you’re not missing out on anything. And the 5-year mark was hard. I’d felt small, but miraculous changes from IVIG and then had an epic autumn backslide that year. The dowsing of that little flame of hope was devastating and it was inconceivable that I would be physically or mentally resilient enough to continue the maybe-I’m-getting-better!-Oh-no-what-fresh-hell-is-this? cycle for years to come.
But, then, suddenly, 10 years have passed. I could almost believe the rest of the world is trapped in amber, frozen in time, awaiting my return. As soon as I kick this thing, I’ll drive back down to the office–each street scene melting and returning into motion as my car passes by–and get back to work. Thanks for waiting, guys.
INFECTIONS
What’s far more unbelievable to me is that I haven’t had a muggle illness in a decade. [Please don’t let this jinx me.] No head cold, no flu, no stomach bug, no chest/ear/sinus/bladder/any-other-part-of-the-body infection. The more time that went by, the more ominous was the thought of contracting an acute virus. For years, I had relentless flu-y symptoms–headaches, sore throats, muscle pain, weakness, chills (and still do, sporadically)–and I have many high out-of-range infection titers*, so the thought of another malady compounding the daily slog was harrowing.
*HHV6 IgG; HSV IgM; EBV IgG; M Pneumoniae IgG; S. Cerevisiae IgG; Varicella IgG and IgM; Coxsackie A7, A9, A16, A24, B1, B2, B5 and B6; Anti Streptolysin O Titer, and Candida IgM and IgA. Yes, really.
Three years into my illness, Dr. Chia told us unequivocally that a run-of-the-mill cold could make me permanently worse, so we have always taken great precautions to avoid exposure, which have only intensified during this pandemic. I honestly wonder if I’ll ever be indoors and maskless with anyone besides my husband again. Even worse, will my husband ever be indoors and maskless with anyone besides me? It’s one thing to choose this life for myself–I’ve made peace with only having remote communication with friends and family; I have a partner and a dog to keep me sane–but my healthy husband’s life has shriveled to keep me safe and the guilt from that is indescribable. I imagine if he weren’t yoked to someone at such risk for serious complications from viruses, he might be out gallivanting and socialising, as well he should be.
VACCINES
One of the first doctors I saw after falling ill said, “You are very sick. We don’t know what’s wrong with you, but you should never get another vaccination as long as you live.” I was confused because, until that moment, I hadn’t linked whatever this sickness was to the flu shot I’d gotten a week before Halloween. I was also confused because, in my healthy ignorance, I thought vaccines only bolstered your immune system. I really didn’t understand, in certain unique circumstances, that they could break it. I used to get every immunization available in an effort to protect myself.
Before I traveled to Central America, I was vaccinated for polio, live typhoid, hepatitis A and B, tetanus, diphtheria and gammastan–all on the same day. In the years after, I got the live varicella vaccine, the 3-shot hepatitis B series, measles, mumps, and rubella and, of course, the flu shot every year, along with a pandemic flu vaccine (H1N1) when they were offered. I didn’t get majorly sick while traveling, I didn’t get chicken pox when I tended to my horrifically poxy husband and I never got the flu despite working very long hours in restaurants, among infectious people (note to the public: restaurant staff work when they’re sick; you have to be on death’s door to ask someone to cover a shift), so I guess the vaccines helped… until they harmed.
COVID
There’s such polarization these days when it comes to covid vaccines. There’s a lot of hatred directed at those who are trying to protect themselves and others by getting vaccinated and wearing masks and there is an equal amount of contempt directed at anti-vaxers. I have yet to see a single news story talk about those of us who want to get vaccinated, but cannot. Or those of us who have to make the agonizing decision to live a life of extreme isolation or risk very serious repercussions from a vaccine–any vaccine. I wish individuals would always take the collective into consideration and try to protect those that are vulnerable, but that’s not human nature, unfortunately. People will refuse vaccinations or not wear masks or not get tested because they don’t want to quarantine. And, all the while, those of us with weakened, damaged or overactive immune systems–be it from chemo or old age or autoimmunity or ME/cfs or steroids or stress or another condition–will have to choose seclusion over risk.
Against one of my doctor’s advice, I will be getting the first covid vaccine next month–but I’m getting a pediatric dose. We will see how I do and then I’ll get a second dose and test antibodies. They will be keeping me for observation in the clinic for an hour because of my history of anaphylaxis, but that’s not what I’m worried about.
I’m worried about being bedbound again. I’m worried about volunteering for an injection that could further damage my autonomic nervous system and intensify dysautonomia and hyperadrenergic symptoms. I’m worried about triggering more vasovagal collapses or making myself more hemodynamically unstable. I’m worried about a cytokine storm and/or a mast cell meltdown that creates a permanent worsening of reactivity when I’m already so limited in medication options and trying so hard to keep on weight. I’m worried about a blood clot causing sudden death because IVIG, oral hormones and inactivity already put me in a high-risk category. I’m worried about losing the limited amount of independence and mobility I have now (but it’s enough for a happy life) and becoming too weak to even wash my hair again. I’m worried about being that burden to my husband again, especially now that it takes so much work to make my GI tract function–it would be a monstrous task for him to take on. Mostly, I’m worried about once again losing the small joys, like taking Penny on our scooter walks, being able to talk on the phone for hours and laughing. I spent years without those gifts and I’m not sure I can claw my way back over another decade.
It feels good to write out those fears. There are very few people with whom I can have these discussions because not many healthy friends understand the risks involved when dealing with such complex conditions. Everyone in my family has had at least 2 covid vaccinations with no side effects, but, in my support groups, it’s a different story. Even there, though, I am careful–I want everyone to get vaccinated, if they can safely, and I never want to dissuade others by voicing my concerns. And doctors aren’t much help because the vast majority take the practical stance that, statistically, the chances of negative repercussions are low and that the risks outweigh the benefits. That’s absolutely true for the typical bell curve of the typical population. Not true for me.
Let’s just hope it’s all smooth sailing. I’d like the next decade to be different.
Update: My doctor pretty much talked me out of getting the C vaccine. I’m too high-risk for long-term reactions. I’m going to have to get surgery next year, so not being vaccinated in a hospital setting adds another layer of fear, but I won’t be stable enough for surgery if the vaccine caused damage. So I will be remaining in strict isolation and putting my life in other people’s hands.
I’m going to try to write something. An update of sorts. Not necessarily because today is exactly nine years since this illness stepped into my body and started controlling the trajectory of my life, but more because it is a quiet Saturday and I can’t call any clinics and I don’t have any medical appointments. It’s Halloween, but we’re completely ignoring it this year. It’s a beautiful day, but I woke up after five hours sleep with bad brain symptoms, so I’m not up for going outside or calling a family member or washing my bed clothes, which are in dire need. And I’m just so tapped out on research right now. Endless, endless research into treatments and specialists and ways to bankrupt ourselves on nifty devices that might miraculously give a reprieve from symptoms or plateau my decline in functioning.
I often don’t write — even if I have the time and energy — because I feel like I want to express something meaningful and express it beautifully, or at least express it well. Express it in a way that others might identify with it or even be moved by it. Or, if not meaningful or moving, I’d like to be able to write something informative. But that takes more mental energy and creativity. I always find a reason not to tap into the emotions that are necessary to write deeply and thoughtfully. I stay sane with distraction, coasting along a wave of TV shows and dog cuddles, trying not to look into the depths below. I’m finding distraction harder this year.
After five years of a slow, but fairly steady increase in functioning, I’ve gone downhill. Not because my dog died or because wildfire smoke was choking us for weeks or because I can’t see my family and my one friend who kept me sane by visiting regularly. And not because of the emotional toll of the pandemic and the rage and heartbreak caused by the political strife in the world. That’s all just icing on the distress cake. The actual bulk of my cake is made of pain, exhaustion, reactions, and failing organs and bones, with thin, bitter layers of isolation and future worries between the tiers of sponge. It’s a really unpalatable cake.
When I first met my friend Jak over at Mast Cells & Collagen Behaving Badly, she had been through ME, then she was dealing with mast cell disease and her body had started to have problems from EDS (Ehlers-Danlos Syndrome, a connective tissue disorder). Most people I’ve met with this illness trifecta started having mast cell reactions after ME hit them. I was the other way around. I’d been dealing with angioedema since I was teenager and I first went into anaphylaxis in 2001. ME hit a decade later. When I met Jak, I didn’t have an EDS diagnosis and, when I first got it, I ignored it and decided it wasn’t true. I remembered, though, that Jak had said, “I could have told you that. With some of your symptoms, it seems obvious.” Her pain and subluxations didn’t start in earnest until she was in her 40s and dealing with peri-menapause, so she cautioned me that EDS could raise its head in the future. No, no, I’m not hypermobile, I said and I ignored it. Well, there’s no ignoring it now.
Last year, I went back to the top EDS doctor here in Seattle and told him I hadn’t believed his diagnosis and could we start from scratch, work me up again, see if he truly thought I had EDS? He smiled (good doctor), he agreed (did another physical exam), he reiterated that I had EDS and showed me what my body is not meant to do. He also diagnosed thoracic outlet syndrome (TOS). For all my research, there are so many odd things about my body that I barely notice. It’s like whack-a-mole — I’m just trying to push down whatever the most concerning thing is on any given day. What do I care if I can’t hang my clothes up or hold my phone to my face without losing circulation through my arms and having my hands go numb? It’s really not important in the grand scheme of this illness. You adapt. So when the doctor asked me if I felt anything as he manipulated my arm, I said, “Nothing. Except there’s no blood flowing and I have pins and needles.” He smiled gently again. “That’s not nothing. That’s what I’m looking for.” It took a very long time for blood to come back into my forearm and hand after whatever he did and I had electric zaps for hours. That was a year ago and I still haven’t read about TOS or whether those symptoms are normal or what to do about them. I don’t really care right now because I’m too busy trying to whack bigger, louder moles.
My leg pain has gotten much worse. I can’t stand in the kitchen to cook as long as I could before and, anytime I do, I have to wear compression stockings and a back brace, but still need to go to the couch and lie down with my feet up after a short while, groaning with the effort. My neck and back have gotten worse. Something in my thoracic spine keeps going out and my lower back and tailbone have a constant steady ache. My neck always feels unstable, so I move it very gingerly, but it also always feels like rebar, so I try not to immobilize it. I pull a different shoulder or neck muscle seemingly every day, usually from thrashing around in bed (unfortunately, not in a fun way, not when I’m conscious). I’m currently ignoring a jaw ache and maybe a cracked tooth from clamping in my sleep and the fact that my eyes never stop burning and are sore when I move them. My left patella keeps shifting out of place and it’s agony when it happens, so I’ve been doing a deep-dive into knee braces and kinesiology taping. I broke my wrist and finger this summer when Penny lunged at an off-leash dog and snapped my hand behind my mobility scooter seat. I’m still wearing a cast or a brace a full three months later and my right hand, which picked up the slack when I couldn’t use my left, has developed instability in the wrist and a subluxing thumb. When my endocrinologist heard about my fractures, she said we needed an appointment asap because she is very concerned that my osteoporosis has progressed. She’ll probably suggest I take more drugs. 🙄
And really none of this is that important because it all pales in comparison to my bowel hell. Bowhell.
Warning: lots of talk about poop and toilets ahead. Enemas barely work anymore. To have a bowel movement, I have to use a liter of water and massage my abdomen for sometimes hours each day. And “massage” sounds delicate. It’s not. I often worry I’m going to rupture something with my squeezing. With my broken wrist and finger, I couldn’t manage to press my abdomen properly for weeks and my bowels suffered. I couldn’t evacuate effectively, which meant I couldn’t eat enough and I didn’t sleep properly. Everything has a cascade effect.
Compounding my bathroom issues is how difficult it is to sit on a toilet. I lose circulation in my legs very quickly (even with a Squatty Potty) and it is incredibly painful on my neck and back. My doctor asked me when my neck was the most painful and I realised it is sitting on the toilet because I have no support for my spine and nothing to lean back on. I’ve resorted to using a hard neck brace (only sometimes — sometimes it makes it worse) and putting a chair in front of me to lean my forehead against, but, even so, after I’m done, I have to lie flat on the floor and, if I have the energy, use heat, traction and ice to help the spinal pain. I was never conscious of just how much I need to support my neck until two years ago when my mother was visiting and I’d made enough improvements energy-wise to go to the opera. Wow, three hours sitting in a short-backed chair was excruciating. I was almost in tears. I was dizzy, my heart rate was high, my legs were losing circulation (I’m short, so I was using my backpack as a foot stool) and I could not hold my head up.
So, sitting is an ordeal. And shitting is an ordeal.
I have a long history of vasovagal collapse from abdominal pain. In my twenties, it happened with the onset of my period because of severe dysmenorrhea. Shockingly, when I got sick, my cramps virtually disappeared. But they’re baaacck! And my period often likes to come three times in one month, so this cramping and inflammation, coupled with random pelvic floor spasms, coupled with colon pain has been a lot. Last June, I sat up in bed one morning and some deep part of my lower abdomen spasmed and I immediately went into a vasovagal episode. My heart rate went so low, that I was having trouble breathing. My blood pressure dropped, too, but the main problem was the bradycardia. I was shaking all over and trying not to black out, but after about 20 minutes, I had to call the paramedics. Before they even got here, the pain abruptly ended and, instantly, my heart rate came up and I could breathe again. (I told them not to come inside because of covid and I gave myself IV fluids at home. I’ve dealt with this before, emergency rooms really can’t help.)
From that day forward, every day for six weeks, I was in an acute bowel pain crisis. I couldn’t seem to eat anything that didn’t contribute to the pain across my transverse colon, I lost weight, I wept each evening, I slept poorly, my attention was never not on this organ that was constantly yelling at me that something was wrong. I wound up getting a CT scan (a big deal during covid and when I’ve had so much radiation in my life) and blood tests because I thought: what if this is life-threatening? I was spooked by a fellow EDSer’s emergency surgery for a ruptured bowel and resulting colostomy bag, but I was even more concerned about the possibility of an elemental liquid diet or a feeding tube. I’ve gone to great lengths to keep a varied diet, not only because food is my one joy besides dogs, but also because I know so many people who never got foods back after strict and prolonged eliminations. And feeding tubes — I never want tubes of any sort stuck in my body, too many complications. It’s the reason I’m still doing weekly peripheral IVs after five years, rather than getting a port or PICC (I don’t know anyone else who has come close to tapping veins for this length of time).
The CT scan showed nothing except my big lunch and tampon (a mortifying radiology report: unremarkable, TAMPON, unremarkable, unremarkable, COPIOUS AMOUNT OF INGESTED MATERIAL IN STOMACH, unremarkable etc…) and the acute bowel pain eventually faded back to my regular constant ache with periodic stabbing knives and electric zaps. But it sure got my attention.
I started Motegrity, a selective serotonin type 4 (5-HT4) receptor agonist, which cost $265 for one box (bought online from Canada because my insurance balked) and then caused possibly the worst medication reaction I’ve ever had. I started Linzess, which cost $350 for one bottle and either causes nothing to happen or a full day of sharts. I’m still taking Iberogast, Miralax, BPC-157, SBI Protect, Thorne SF722, oregano oil, berberine, magnesium, digestive enzymes, betaine HCl, and probiotics… all for my bowels. I’m about to try Mestinon, LDN and Cromolyn again (okay, I take it back, the latter was actually the worst medication reaction I’ve ever had — and I’m going to try it again, which has to show my level of desperation); these are all medications that can help motility. Plus, I have a Xifaxan prescription at the ready (which I’ve already taken twice) when I’ve exhausted all of these options.
It’s a next level problem. What I mean is, there were four years in the beginning of this chronic illness when I was “just” dealing with ME and MCAS — when I could still poop! When it was “just” muscle pain, but my joints were fine and my bones felt sturdy. Unbelievably, there were years when I didn’t have brain symptoms. I had the low-level kind of brain fog that made you forget things or not be able to find words, but, in the beginning, I didn’t have the buzzing brain and eye pressure, slurring and screaming tinnitus that makes bed the only possibility, even if my body is feeling strong. These new additions take illness management to the next level.
I’m on my third gastrointestinal doctor. The first said: Miralax, papaya, probiotics. Huh? Did you even hear the part about dead colon? On a return visit, she said: Daily enemas for life. Are you fucking joking? I asked her when she would recommend a colonoscopy (back before I realised it would need anesthesia in my case). When you have bloody diarrhea, she said. Right. Okay.
The second GI doctor said: Colonoscopy and endoscopy. On a return visit, she said: COLONOSCOPY AND ENDOSCOPY. She would not talk about any other tests or interventions. I don’t want to go through that. I don’t think those procedures will show anything and, with my medication reactions, there are legitimate risks to full anesthesia, not to mention the clean out having risks because of my hypotension and hypoglycemia. I thought (and still think) that it was prudent to exhaust less invasive options first.
These two doctors were young women at the University of Washington, one touted as The Motility Expert and the other as being EDS-knowledgeable. I mention this because I would assume I would be most comfortable or have the best experience with them instead of the third GI doctor, who is an old man that made a slightly misogynist comment right out of the gates and doesn’t make much eye contact. But he has been the only one to think outside the box and marginally help me. He ran tests that nobody has ever run since I’ve been sick (I’d never had a stool sample done or celiac test!) and spent 40 minutes discussing my mast cell history before even broaching the subject of my bowels. He dismissed a colonoscopy and it felt like he’d lifted a 100-pound weight from my shoulders because I was crippled with guilt after rescheduling the procedures over and over for a year and a half.
So, because of the progression of bowhell symptoms and structural issues the last few years, I have been pursuing MRIs and neurosurgical consultations. A cine CSF (cerebral spinal fluid) flow study showed a lack of CSF in my hind brain, caused by low-lying cerebellar tonsils (LLCT). My neurosurgeon (who is experienced in dealing with EDS/MCAS/ME patients) also suspected craniocervical instability (CCI), but couldn’t recommend surgery from my MRI measurements and symptoms without first performing more tests (invasive cervical traction (ICT), where they lift up your skull with a pulley system to see if there is an improvement in symptoms, and intracranial pressure monitoring (ICP ), which is a bolt in the skull that holds a probe that measures pressure in your head while concurrently preforming a lumbar puncture). I decided not to do either of those because, as you might have guessed, I don’t like rocking the boat (with, say, a new soap, let alone invasive tests that involve holes in my skull) (oh, and travel across the country) (and covid). But I have wondered if the blocked CSF flow is contributing to or entirely causing my brain symptoms. That’s a big deal. I used to feel smart and effective.
But the biggest deal of all came from the neurosurgeon looking at my pelvic MRI defecography from five years ago (which I didn’t even send to him because I was only consulting him about my neck; he must have gotten it from my specialist, who was the referring physician).
“You have a large bowel,” he said.
“I’m not surprised.”
“And what have you been told about your enormous bladder?”
“My what?” He has a thick Italian accent straight out of central casting and I didn’t know there was anything abnormal about my bladder.
“Your enormous bladder. Your ENORMOUS BLADDER!”
He had to repeat it four times before I could understand what he was saying. It was pretty comical. Nobody had ever mentioned my bladder. He recommended a renal ultrasound to rule out hydronephrosis, urodynamic testing for neurogenic bladder, and a lumbar MRI to look for tethered cord. I’m sure you’ll be shocked to know, I ignored it all… until I watched online presentations by Petra Klinge, probably the top tethered cord specialist in the country, and a Q&A with Dr. Klinge and Jeffrey Greenfield where they mentioned that, although bladder symptoms are the hallmark of pediatric tethered cord, in adults it’s often bowel problems, usually constipation. Ah.
I sent my lumbar MRI (both prone and supine) to my neurosurgeon and he diagnosed “tethered cord, classic variant,” which is notoriously hard to see. In other words, as my complex disease specialist emphasized to me repeatedly, it is rare for this neurosurgeon to diagnose tethered cord before CCI from a lumbar MRI. This is the case even though they have both actively been trying to identify it early since so many of their patients have to return for a second “detethering” surgery after undergoing craniocervical fusion.
“Elizabeth, why aren’t you on a plane to New York for SFT [sectioning of the filum terminale]?” my specialist asked me.
Friends, I DON’T WANT SURGERY. EVER. No surgery, but ESPECIALLY NOT SPINAL SURGERY.
I will leave you there. We have much to discuss. This is now my focus. I need to do everything I can to manage these symptoms and to halt their progression. Meds, exercises, physical therapy, prolotherapy, I don’t know what. Right now, my plan is to plan. I’m not willing to see any healthcare practitioners in person, so it’s tricky, but it’ll be a winter of research and putting some ducks in a row.
I also have to start preparing for a what might be an inevitable surgical eventuality. I need a pain management protocol with bigger guns than paracetamol, I need to strengthen my core and my bones, I need to find muscle relaxants to which I don’t react, I need to get my blood pressure up and control my MCAS as much as possible. I need to save money. No more ignoring.
Happy Samhain, everyone. And my 9th “sickiversary” — not a happy day, but one that should be acknowledged, nonetheless.
I want to talk about my success with IVIG (intravenous immune globulin) since this is something that I am frequently asked about by other patients. I’m in a very unusual situation where I administer my own IVIG and fluids through peripheral venous lines (not using a port or PICC) at home without a nurse. I feel extraordinarily fortunate to have been able to get this treatment at all, but it feels particularly fortifying during this pandemic. Not only because I am receiving a protective, difficult-to-access medication, but also because, when covid hit, I was in a position to continue treatment uninterrupted in my home without needing nursing visits that would increase my risk of exposure to the virus.
It’s also unusual that my IVIG is prescribed by a naturopath, rather than an MD (let alone an immunologist), and that I do infusions once a week rather than every 3 or 4 weeks, and that I was approved for a high ‘immunomodulatory’ dose without having one of the autoimmune diagnoses that is typically needed and without having to do a vaccine challenge. Also, I don’t have side effects from IVIG, which I find miraculous, but I think it is because of how careful (and controlling) I’ve been throughout the whole journey. I researched and advocated for myself at every turn — undoubtedly more than was really needed — but I have no regrets since it has been such a godsend and I’ve had no bad reactions.
The story starts when I went to see Dr. Chia in 2014 (almost 3 years after getting sick) and he ran a bunch of blood tests that no other doctor had bothered to explore up until that point, such as HHV6 and Coxsackie antibodies, T-cell counts, and total IgG with subclasses.
For anyone navigating the newly-sick morass, I want to point out that I had seen over 30 doctors in those first 3 years, trying desperately to find one big brain that might have some insight. Infectious disease, endocrinology, neurology, allergy, cardiology, rheumatology, sleep doctors, ENT, gastroenterology, functional medicine MDs — you are shunted from one specialty to another to another with no one willing to dig deeper. I am even including appointments with my OBGYN, ophthalmologist and acupuncturist in that count because I was chasing down every lead I could (maybe it’s all hormonal, maybe my eye pain will lead to a brain discovery, maybe ‘dark yin’ is my problem after all). The big issues were missed until I was able to see Dr. Chia and Dr. Kaufman (ME/cfs specialists in California) and — this is the part for anyone who might be overwhelmed with where to start — a local naturopath (ND). In fact, the best help I got in Seattle was from two different NDs: they thought outside of the box and dug a little deeper, like the specialists. And I don’t mean woowoo shit, I mean things like checking for an immune deficiency DUH since I keep telling you it feels like my immune system just broke one day. Soon after I traveled to California to see Dr. Chia, I found an ND who ran almost the same battery of tests which revealed the same abnormal results. The first ND, who agreed I needed IVIG, but couldn’t get it for me, tried a bag of different tricks aimed at increasing my IgG levels. They didn’t work, but I was very grateful to have someone try something. Point being, if you can’t see a specialist, I would advise finding an ND who will look at your immune system health and infections and who is willing to walk the long road with you, being patient while you try (and, in my case, most often fail) different treatments.
But, I got ahead of myself. Dr. Chia saw that my total IgG was low and so were some of the IgG subclasses. He said I needed IVIG, but he didn’t offer to get it for me (I thought at the time it was because he was in California, but I now know Seattle patients that get IVIG through Cali doctors, so I’m not sure why he couldn’t have ordered it). Once I was back home, I asked my 4 doctors if they could help me get IVIG (primary care doctor, rheumatologist, endocrinologist, ND) and they all said no. My PCP did go a little further by asking an immunologist colleague, but he said my IgG would need to be lower or I’d have to do a vaccine challenge, which I refused.
I had given up and stopped asking when I found my second ND (who was very different from my first; both have been helpful in separate ways). The very first thing she said after entering the room on our first meeting was: “You need IVIG.” She had reviewed my lab work (she had reviewed my lab work!! I don’t think any other doctors had actually looked at anything ahead of time) and seen that my IgG was continuing to decrease over the months. I had hypogammaglobulinemia and fit the diagnosis for common variable immune deficiency (CVID) and she was confident insurance would approve immune globulin therapy.
Between that day and my first infusion, 11 months went by. I delayed until I felt I had thoroughly prepared in every way to keep myself safe. Anaphylactic or anaphylactoid reactions can occur in any patient receiving IVIG therapy, but I had a history of both (plus intractable migraines), so I was nervous and wanted to control every aspect of treatment. My doctor was patient and accommodating. I don’t think any other doctor would have let me take the time to tackle each concern and build up the confidence to take the plunge. I think of it a little like a lost year when I could have been feeling better, but, like I said, I really can’t have regrets when things went so well.
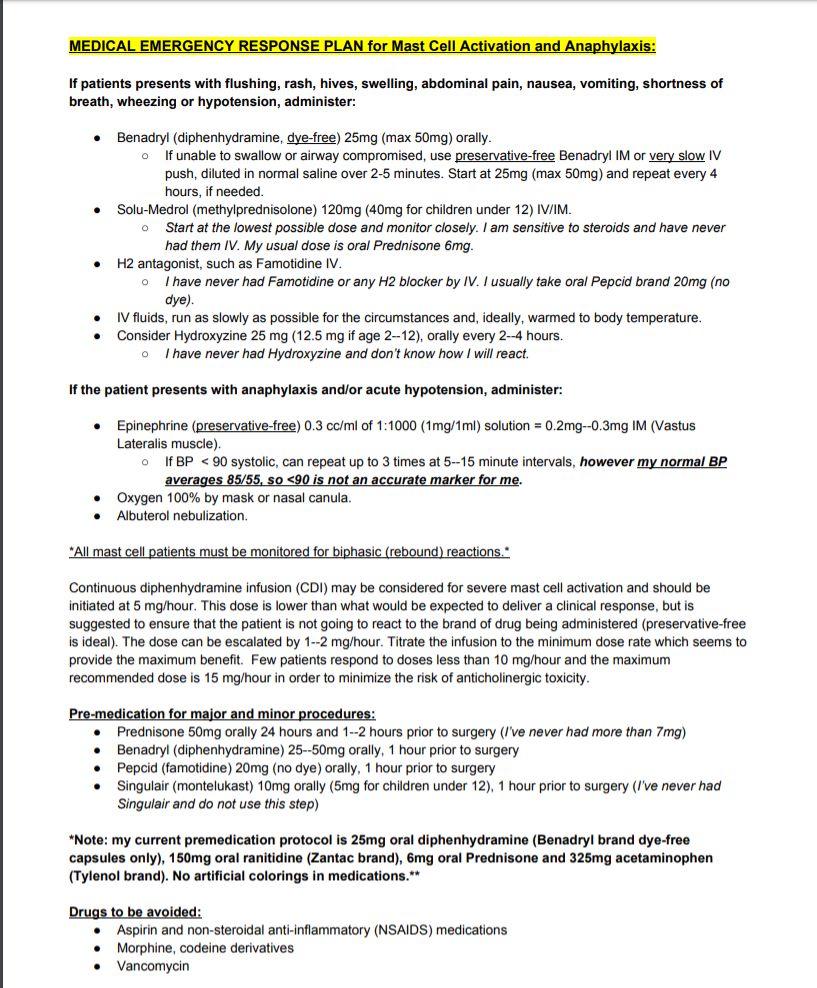
First off was figuring out how to safely take pre-medications for potential reactions to the immunoglobulin and how to get IV fluids (which would be administered before IVIG) without side effects. I was extremely reactive back then because of out-of-control mast cells and I had no safe rescue medications or pre-medication protocol. IV fluids had caused angioedema and breathing issues; I was so sensitive to Benadryl, I couldn’t even take drops without feeling anticholinergic-type symptoms; tiny crumbs of steroids made me feel like was hit by a truck, running on a treadmill and sedated all at once. I didn’t feel comfortable doing IVIG without having a rescue protocol, so, during that year, I worked on my tolerance and put together a safe plan.
First, my doctor put me on bioidentical hormones because there is some evidence that they can help with mast cell reactivity. Then, we tried IV fluids, but only 250 mls, warmed up and run at a snail’s pace (my previous reactions were from 2,000 mls of cold fluids run very quickly on the day my period was due (when I’m highly reactive); I didn’t know any better). I even found out I was fine with two types of normal saline bags, but not another. I slowly gained tolerance to Benadryl (dye-free capsules, only) and Prednisone (finding manufacturers with the cleanest excipients), taking bigger and bigger slivers until I knew I could safely premedicate before infusions. Those that know me understand that the symptoms that have scarred me the most are my mast cell reactions. They are unpredictable and violent. Full-blown anaphylaxis almost killed me. I can’t adequately express how jubilant I was to have a safety net, to have protection, to be able to put a protocol on paper that anybody could follow in case of an emergency and to have tools with which to arm myself before a procedure. Having intolerable side effects from the things that are meant to counteract intolerable side effects was a scary place to be.
Next, I talked to my doctor about starting with subcutaneous infusions (SCIG), rather than intravenous because all of my research indicated that the former was safer. She agreed, thankfully, although she gently pushed for IV for years after that. I also asked if I could start with 1 gram at a very slow rate of delivery and she acquiesced to that, too. NO allopathic immunologist would have agreed to that EVER.
Then I looked into a hospital infusion versus an ambulatory infusion suite (AIS) versus at-home infusions. I was told a hospital wasn’t an option and the AIS was staffed only with a nurse, no physician. If I had a reaction, the protocol was for the nurse to administer supportive meds and call 911, if needed. Well, staying at home was a no-brainer. I would have a nurse in my house, but, more importantly, I feel much safer with my husband there as an advocate. Plus, we live very close to an emergency room and he could whisk me there if calling an ambulance didn’t feel like the appropriate move. In the past, we have sat in our car in the ER parking lot, waiting to see how reactions progressed. The high price of healthcare in this country is a great deterrent.
Then I wanted to look into IgA deficiency. There is some research that low serum IgA and anti-IgA antibodies increase the risk of anaphylaxis and the remedy would be to use a very low-IgA brand of immune globulin for my infusion (says my Labcorp test result: “Patients with IgG antibodies against IgA may suffer from anaphylactoid reactions when given IVIG that contains small quantities of IgA. In one study (Clinical Immunology 2007;122:156) five out of eight patients with IgG anti-IgA antibodies developed anaphylactoid reactions when IVIG was administered.”). My total IgA and one IgA subclass had been low in the past, but neither my doctor nor the infusion pharmacist suggested that this should be a consideration — I had to get the info from other patients and insist (nicely) that we test my anti-IgA antibodies. Gamunex-C was the brand that had already been approved by insurance and I knew that I was very lucky to have it and might lose it if we had to resubmit an authorisation, but safety first. Gammagard could have been a safer choice since it has extremely low IgA content. It took an excruciatingly long time to get those results but, ultimately, I did not show anti-IgA antibodies, so we pressed ahead with Gamunex. And I’m glad we did! One of my nurses commented that it is the “top shelf” immune globulin and it’s been good to me.
The final hurdle was scheduling. Back then, I was much sicker in the mornings — shaky and very low blood pressure — but that is the time of day when nurses typically arrive for long appointments. I always thought, if I became a home infusion nurse, I would offer nights and weekends, just like my preferred shifts in the restaurants. There must be more patients like I am whose vitals stabilize as the day goes on. Also, my period was looming, a time of the month when I am highly reactive, so I wanted to avoid that whole week (although this wasn’t as easy as it sounds because my cycle wasn’t/isn’t regular). The day came when things eventually fell into place and my wonderful nurse, Marie, came to my house to hook up the IV fluids and teach me how to infuse subcutaneously. She showered beforehand and changed her clothes because she and some of her other patients have cats. She understood my nervousness and didn’t rush me or complain even though she had to sit in one room with me in a straight-backed chair for 8 hours. Marie came every week for 16 months to hook up my IV, but, once we knew I was doing well on this treatment, she was able to leave quickly and I would disconnect my IV fluids and do the SCIG myself.
We started with 1 gram infused through a 2-needle set and F30 tubing. That probably made anyone knowledgeable with immunoglobulin infusions laugh because it is SO SLOW. Like, unheard of. My nurse had to do a special order for the supplies because they are normally only used for infants. Over the weeks, we slowly worked up to 5 grams (eventually using a 3-needle set and F45 tubing — only slightly faster), which is a typical ‘replacement’ dose for a primary immune deficiency patient of my weight. I stayed there for a year and a half, not pushing my luck in any way. Slow and steady.
In 2017, a miracle: I switched infusion companies from Coram to Accredo (with nothing to which to compare Coram, I thought they were fine, but things have been much better with Accredo) and they suggested I learn to insert my own IV catheter for fluids. Uuh, yes, please! Actually, they suggested my husband do it, but he’s not good at these things and I am, so a nurse came over and gave me a tutorial and that was that. I was only “allowed” one training session, so I wound up watching a ton of YouTube videos, which is why I’ve now made my own, in case they can be helpful for anyone.
For over 3 years, I’ve been placing my own peripheral IVs each week. It gets easier and easier and, honestly, I feel so much safer. Although Marie was very careful, I am more careful because I have a bigger stake in the game. I do not want to ruin any veins or get an infection, so I am vigilant (and superstitious) about my aseptic technique and I rotate veins to give them a break. Every single week, for the entire 16 months that Marie was my nurse, she used the left median cubital vein (antecubital or, as my nurses called it, the “AC vein”). I never questioned it because it held up well, but that’s about 60 catheters inserted in the same place (what a trooper my vein was!). As soon as I was doing it myself (and discovered I was ambidextrous when it comes to IV placement), I started using a different vein each week. I have 6 sites that I use, but 2 of them (on the outside of my forearms) are difficult — the veins roll and there’s always more of a risk of having to do multiple pokes — so I use the cephalic and AC veins more often than not, even though it means having to keep my arm straighter. I don’t use my hands or wrists, partly because I wash my hands so often, it’s an inconvenience and partly because I want to save those sites for easy access if I’m ever in the hospital with a nurse that needs fat veins for larger gauge needles.
Holy roller
Then in 2018, another miracle: I switched from SCIG to IVIG and was able to continue to do it myself at home. Not only that, but I was allowed to continue infusing once a week, which kept my levels more consistent with fewer peaks and troughs, which in turn kept my energy more stable. IVIG is typically given every 3 or 4 weeks for multiple days in a row, necessitating a peripheral IV be left in place for 3 or 4 days (I can’t even imagine; 12 hours feels like an eternity). This is one of the reasons so many people get PICCs or ports.
I am regularly asked how I managed to get self-infusion approved at home. I didn’t do anything. I didn’t even know it was something that was allowed. I lucked into it with a good doctor, a good infusion company and a good nurse.
The first year I was with Accredo, I had increased my SCIG dose from 5 grams to 10 grams. My legs (my preferred place for the subcutaneous needles) weren’t happy, though. They weren’t absorbing the medication as well as they used to and they were swollen and sore for longer afterwards. I was using 6-needle sets to try to stop leaking and I felt like a pin cushion. I also wanted the option of trying high-dose IgG (my specialist had said for years that I needed 20 grams/week) in the remote chance that insurance would approve it. So I talked to my doctor about changing brands to one with a higher concentration, which would mean less fluid infused into my tissue. I was still adamant that I didn’t want to try IVIG. I didn’t want to tempt fate and I was scared of medications going directly into my veins and causing an instant reaction. My doctor pointed out that my body liked Gamunex, so I could either stick with what we knew didn’t cause a reaction (because Gamunex can be infused by either route) or stick with SCIG and change brands. I decided that it felt safer to stick with the brand I knew and loved, so IVIG it was.
They sent a home health nurse to do the first IVIG infusion. I had already placed my IV catheter and run my fluids when she arrived and she said it was perfect. Once again, we started at a low dose (2.5 grams) and ran it very slowly. We worked back up to 10 grams a week over a few months. During this time, I changed from the first awful, bullying nurse to one I adored (we could be friends in a different life). Jennifer showed me how to run the IVIG after the fluids and made sure I did everything right, but one week she said, “I’m just a fly on the wall. You place the IV, you run the fluids and medication, you disconnect. There’s no point in my being here.” So she recommended to my doctor that I do it alone under the condition that I have a responsible adult available at all times during an infusion in the case of anaphylaxis. That’s how I wound up doing it without a nurse and I’ve never met anyone else who is in this same situation.
The final miracle happened this year: My insurance approved the high dose IVIG (20 grams a week, which works out to almost 2g/kg/month, what is considered autoimmune or immunomodulatory dosing). I’m not sure which of my ridiculously high titers got it authorised and I’m not going to question it, I just thank the universe each week and try to keep finding the money (my 20% copay is $1,400/month). I increased slowly over months and had some headaches in the beginning, but nothing now. I am energised the day after. It’s like liquid life-force. I only premedicate with 25mg Benadryl, 20mg Pepcid and 4mg of Prednisone and I could probably do less. The number one benefit to doing it solo is that I’m able to program the flow rate as slowly as I like, which ameliorates side effects. If I had medical oversight, I’m sure they would insist I increase the rate, if for no other reason than to get the nurse out of here quicker. Talking to friends who have dealt with aseptic meningitis or incapacitating migraines, it seems to me that flow rate being too high is the major precipitating factor.
IVIG changed my life. I started the first wee tiny dose on October 2nd, 2015 and improvements in ME symptoms happened very quickly. By January 2016, I felt confident enough to write about them. They marked the end of 4 years of a steep and terrifying downhill trajectory and the beginning of a very slow, but steady uphill trajectory for the past 5 years. There have been lots of setbacks, plateaus and crashes (scary ones and months-long), but, overall, I’m stronger and more able-bodied each year over the last.
There are so many things I’ve learned along the way that I want to share like: try to get shelf-stable bags of fluids. My first pharmacy removed the air from the bags of saline before sending them and I didn’t know that there was another option. Once the bags have been accessed to remove air, they have to be refrigerated and thrown out after 14 days. They take up a lot of room in the fridge, it take ages for them to come to room (or body) temperature and you can’t have extras on hand when they’re considered unsafe after a few weeks. My bags now can be stored at room temperature in my closet and their expiration dates are years away, which means I have them for emergencies and don’t need to go to the hospital if all I think they can do for me is administer fluids (which is what has happened so many times in the past with my vasovagal collapses).
This took on even greater importance when covid hit. I feel so lucky to have extra supplies and the ability to give myself IV fluids without going near healthcare facilities. When I’m doing the clean-out for an upcoming colonoscopy, my doctor wants me to give myself IV fluids, which I wouldn’t have been able to do without this lucky situation. And when I imagine the big earthquake or an end-of-world emergency, it gives me solace to know that I am trained and my home is so well equipped.
I’ve also learned that I never want to use gravity tubing and an IV pole when a pump and carrier bag is so much easier, safer and more precise. I don’t have to keep my fluids vertical and elevated, dragging a pole around the house; I can walk around with the bag holding the saline and pump on my shoulder like a purse. I’ve even gone to doctor appointments and run fluids in the car during our California road trip last year after a big blood draw.
I learned from other patients to prime the air out of the bags through the tubing before priming the saline (fill the tubing with saline), which seemed slightly safer than the way a nurse showed me using a syringe, which requires accessing the rubber stopper. Uses fewer supplies, too. Less plastic waste.
Medical waste
I called B. Braun, the company that makes my normal saline, and learned how to safely warm the bags before administration, so I don’t react to the room temperature (which is chilly!) fluids. I figured out that running fluids at a slower rate (150ml/hour) cut down on post-infusion headaches and it was even more effective to bookend the Gamunex with 500ml of saline before and after, rather than running the entire liter beforehand.
I learned that I can keep using the pump for 12 hours after it beeps that the battery is low. Again, less waste. (Although, I wouldn’t sleep with a low battery, just in case.) And I learned that the Bodyguard pump’s beeps terrified my dogs because they were too similar to our fire detector, but the CADD Prism’s beeps go unnoticed.
Bad beeper
Wonderful nurse Jennifer gave me a fabric one-handed tourniquet which has made such a difference to my independence and the comfort of my skin. She also taught me that if the ultrasite on the saline lock is going to be unattached for any length of time and I don’t have a cap for it, an old nursing trick is to stick it inside an alcohol prep pad (leaving the wrapper on) and secure it with tape.
Wonderful nurse Marie taught me how to use gauze to support the catheter if it doesn’t lie flush with the skin and how to tape a loop of tubing to your arm, which has stopped my IV from being yanked out many times when I snag it on something. She also always used alcohol prep pads and iodine to clean the insertion site, something which many find overkill, but makes me feel more confident in my infection control.
I learned the catheters with wings are much easier for me to insert than the ones without and that you can ask for sterile gloves rather than relying on the box of non-sterile gloves that they send by default. I learned that you can order sterile pads on which to lay your supplies and IV3000 adhesive dressing that doesn’t tear up your skin like the Tegaderm that comes inside IV start kits.
I figured out by trial and error that some veins need to be stretched taut and stabilised and, if you are inserting your own IV and don’t have two hands, there are ways to do this by twisting your forearm and flexing your hand. I also found out that some veins are close to nerves and your thumb might have pins and needles for weeks afterwards, but they will, thankfully, eventually go away.
During SCIG, I learned that there are handy rate and time calculators for subcutaneous infusions and that if you are having trouble with leaking, swelling, hitting blood vessels etc., that you can try different needle lengths and different needle brands and — the key for me for whatever reason — different needle tops (the soft adhesive ones worked best for me rather than the hard plastic ones that needed to be covered with Tegaderm). I also learned that fat is key to comfort — the medication was much better absorbed if I put the needles in the back of my hips/ top of my butt (saddlebags??).
The most important thing I’ve learned is that although most patients in online support groups ARE NOT MEDICAL PROFESSIONALS AND YOU SHOULD ALWAYS CONSULT YOUR DOCTOR ABOUT EVERYTHING, they are a wealth of information. Doctors and pharmacies didn’t tell me anything about how to manage infusions safely. The majority of my home health care nurses didn’t verbally educate me — it was up to me to observe, ask questions and do my research.
I need help from all the smart people here. Any brainstorming and all ideas welcomed.
This morning I had to call the paramedics because I had another “collapsing episode.” Severe abdominal pain triggered low blood pressure and a very low heart rate. I was shaking violently and having trouble breathing, the latter seemed to be caused by the discomfort in my heart. I fought very hard not to lose consciousness. I was covered in cold sweat and my vision was blacking out. But the bradycardia and trouble breathing were the worst. It felt like my heart might just slow to a stop and I would be gone. It lasted for over half an hour — an eternity while panting with my HR in the low 40s when it should have been twice as fast.
The last time this happened, my doctor ordered a heart workup, which showed nothing, really (I’ve put the results below; I don’t really know how to interpret them). What I’m trying to figure out is if there is anything I should look into besides making sure my heart is okay. I’m on BP medication (to raise it), I don’t have POTS (as in, high heart rate)… I am so wiped out today and I can’t believe I just have to ignore these episodes, shrug and move on. What my heart did today was terrifying!
If anyone wants to help me play medical detective, here is the history of these episodes (no other health history included and there was a lot, obviously).
My episodes, as best as I can describe them, are vasovagal syncope. But they’re more complicated than that. It’s not a faint and then BP recovery once I’m supine. Abdominal pain/pressure/inflammation/cramping/spasm = BP and HR crash.
The first one I remember was in 2005 on the first day of my period. I used to have excruciating dysmenorrhea and one month it caused a collapse — on the bathroom floor, cold sweats, shakes, vision blacking out, very low BP. Went to the emergency room, got IV fluids.
This continued to happen once or twice a year until 2011 — and I can’t predict which months or why. It has happened when my period had nothing to do with it, but it was triggered by my bowels. I have had constipation my whole life, the last time I ever took a laxative was in 2008. The pressure/cramping caused the same low blood pressure, near-loss of consciousness result. My best friend held me up on the toilet while firemen filled my bathroom. As soon as my bowels moved and the pressure released, I recovered.
The only time I remember it not having anything to do with abdominal pain was one of the worst times. I spiked a fever and then collapsed on the front steps to my house and the medics couldn’t get a blood pressure reading at all. Went to the ER, got IV fluids.
I need to mention that all of this was pre-ME. An odd thing happened after ME destroyed my life in 2011– the dysmenorrhea stopped. I went 3 years without a collapsing episode, then had a random one in 2014 and not again until last year, once in February from random severe period cramps on the first day of menstruation (I think it might have been a burst ovarian cyst since it was so out of the norm) and once in July from a massive acute bowel spasm that was about a 9 on my pain scale.
(I should also mention that every time I went into full-blown anaphylaxis was at the start of my period. That started in 2001, four years before the collapses.)
The difference between these recent episodes (last year’s and today’s) and the pre-ME ones is it seems to be more about my heart and less about my BP. Both are low, but my BP isn’t scary-low (scary to EMTs, maybe, but not to me). I used to be able to not talk or move because I was so hypotensive, today I made it downstairs to open the door and had more awareness — was monitoring my HR and O2.
The past few days, I had a deep ache in the very bottom of my abdomen. I cannot have bowel movements and am completely enema-dependent with chronic pain and bloating, so I only noticed this pain because it was so low in my belly and deep-feeling. I kept looking for my period, thinking maybe it wasn’t my bowels, but was instead a heavy, achy uterus. When I went to sit up in bed, the pain skyrocketed, maybe my bowel spasmed like last year. I immediately started shaking and sweating, the vagal reaction happened right away. That’s my best guess — trapped gas in my very dysfunctional, SIBO-ridden bowel created pressure, pain and spasm that triggered a vasovagal response. The pain and bradycardia resolved at the same time and so did the shakes and panting, but I’ve been completely wiped out all day. I’m still in a lot of bowel pain now, 12 hours later, but it has moved up to its normal position in the upper abdominal quadrants.
So, any thoughts? With no period involvement, no actual bowel movement, and symptoms so severe that I called 911 (that is literally the SECOND since being sick — 9 years), I can’t believe I just have to ignore it and go on as usual, without answers. I mean, besides the obvious remove my bowel and remove my uterus, but I’m just not there yet.
*****
Echocardiogram:
There is mild aortic insufficiency. Mild aortic regurgitation is present. There is an eccentric jet of aortic insufficiency directed towards the septum. There is trace mitral regurgitation. Trace tricuspid regurgitation present.
30-day heart monitor:
The vast majority of episodes show normal sinus rhythm without ectopy. Some episodes of dizziness show sinus tachycardia. One PVC and one blocked PAC were observed.
I have to memorialise what happened yesterday because I am astounded and grateful and I bitch so much about the healthcare in this country making so many of us go broke, but this was truly amazing.
On Monday, December 30th, for the hell of it (and prompted by something my friend, Rachel, posted), I decided to ask my brand new doctor (who doesn’t even know me; I was just dumped on her plate when my phenomenal primary care provider left the clinic) if there was any chance we could squeeze in an MRI before the end of the year because I had met my insurance’s out-of-pocket maximum expenditure for 2019 (meaning, in theory, I wouldn’t have to pay for anything else — and wouldn’t it be nice to get the MRI that one of my specialists requested for free?).
Astonishingly, she answered me the same day and said she had put in the order for the MRI, but she doubted it could happen because it needs a prior authorisation (PA) from insurance and that usually takes 8 days or more. I never expected her to read the message during this very busy time of the year, let alone answer it, let alone put in an order without seeing me in person. I was shocked — she trusted what I said in my email! Maybe I should stay with this doctor, after all.
So, yesterday, the LAST DAY OF THE YEAR, at 7:30am, I call my insurance to ask how long it would take to get the PA. They say to call another company, AIM.
I call AIM and they say the PA can only be expedited if the order is marked urgent and mine isn’t (and it definitely doesn’t warrant an urgent request, so I’m not going to pursue that). But they tell me there is a way to get it approved immediately — if the doctor calls them and answers questions over the phone.
I email my doctor to tell her this, making it clear that I understand she probably won’t see the email and wouldn’t have time to call AIM, regardless.
Then I call radiology to see if I can grab a same day appointment, just in case. Radiology Ryan tells me they have one opening left, but I can’t have it unless they have a PA in place.
Then my doctor’s medical assistant emails to say she can’t get a PA without my having an MRI appointment. Well, that’s a catch 22. And she needs a CPT code.
Meanwhile, throughout all of this, I am going to two big doctor appointments — end of year endocrinology and a 2-hour allergy testing for anesthetic agents — sending emails and making calls in between talking to doctors.
As soon as I’m back in the car, around 11:30am, I call Radiology Ryan and tell him my conundrum — that I need an appointment to get a PA. He says their rule only excludes same day appointments, so I can make one for the future just to secure the PA and, if it comes through, call back to reschedule for today. If the spot is still available. Ryan gives me a random January appointment, but tells me the doctor should provide the CPT code. Then, hearing my whimpering, he takes pity and looks up the code for a “lumbar MRI without contrast.”
I email the MA, tell her the code and my appointment date, and cross my fingers.
Soon after I get home, there’s a message from the MA saying she called AIM and got the PA. It’s a miracle!
I call Radiology Ryan. It’s now 1:30pm. He looks for the PA in his system, sees everything is in place, and tells me there’s still a 1:45pm MRI opening. And it’s on a 3T machine, which is what I need. Another miracle!
I shove some food in my face and dash over to the third hospital of the day, which is only 5 minutes away.
The woman behind the desk tells me I have beautiful eyes and my day just couldn’t get much better.
I fall asleep in the MRI (even a few minutes can help!) and then walk over to the medical records office and get copies of my imaging within 15 minutes.
All in all, it was 26.5 hours between my doctor’s MRI order and having my imaging discs in hand.
Mind blown. All of the people who contributed to getting this done deserve wine and chocolates, including the eye flatterer.
Also, after being completely debilitated by head, neck and eye pain for three days, yesterday it completely eased up.
Also, it was a beautiful 7:40am drive downtown, a time that I’m rarely out of bed.
Also, my thyroid levels are dialed in.
Also, all of the skin prick and intradermal tests for medications were negative.
Also, I walked around the hospital by myself for the first time since I used to volunteer there 12 years ago. My husband usually pushes me in a wheelchair.
Also, we stopped briefly at a grocery store and I walked around like no big deal.
Also, the grocery store had tons of good salads in the deli, so I didn’t have to cook.
Also, I succeeded again in inserting my peripheral IV in a hard-to-access forearm vein and it is so much better to be able to move normally throughout the day without worrying about kinking something in the elbow or wrist.
Also, although Penn kept me up most of the night with her fireworks panic, Riley has decided that he’s too old to give a shit and one terrified dog is definitely easier to deal with than two.
Also, I had the best Christmas health-wise since before I was sick. <– This last point is so exciting, it will get its own blog post.